 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
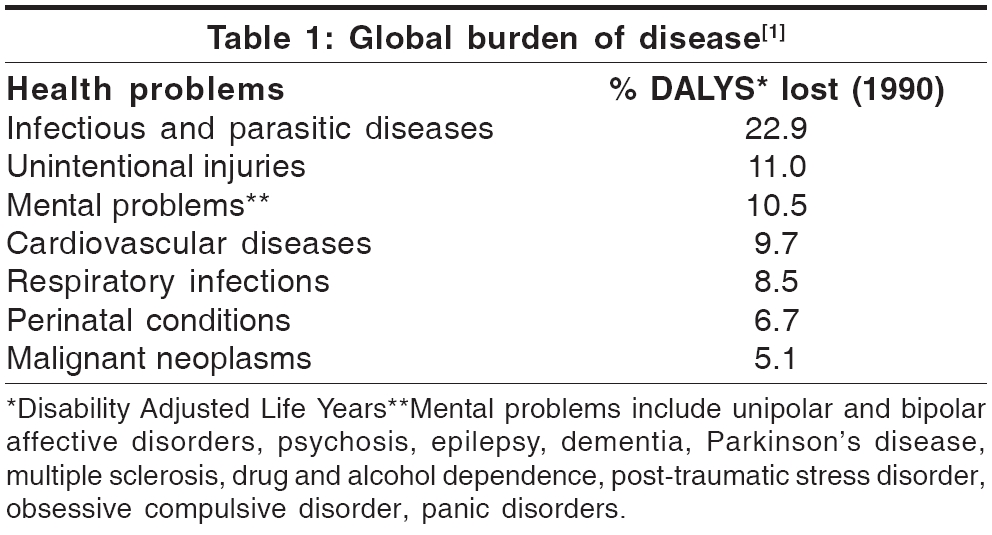
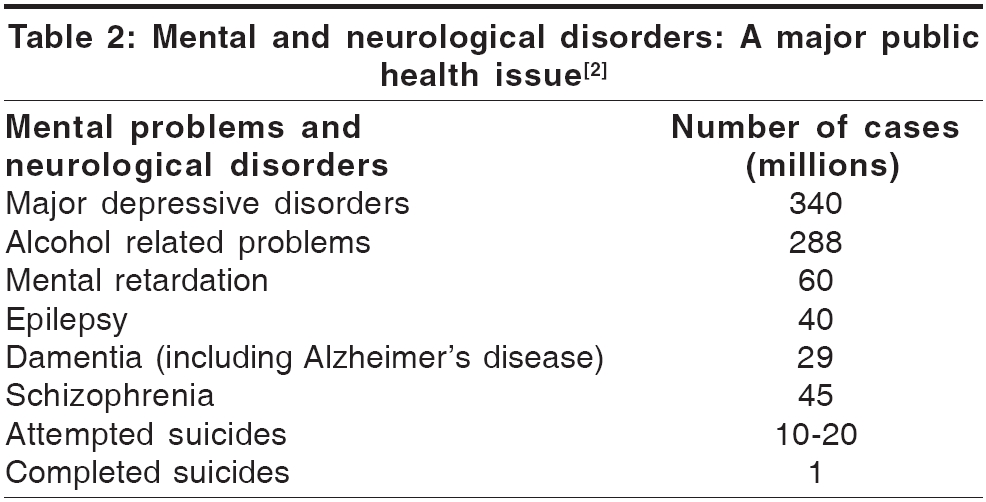
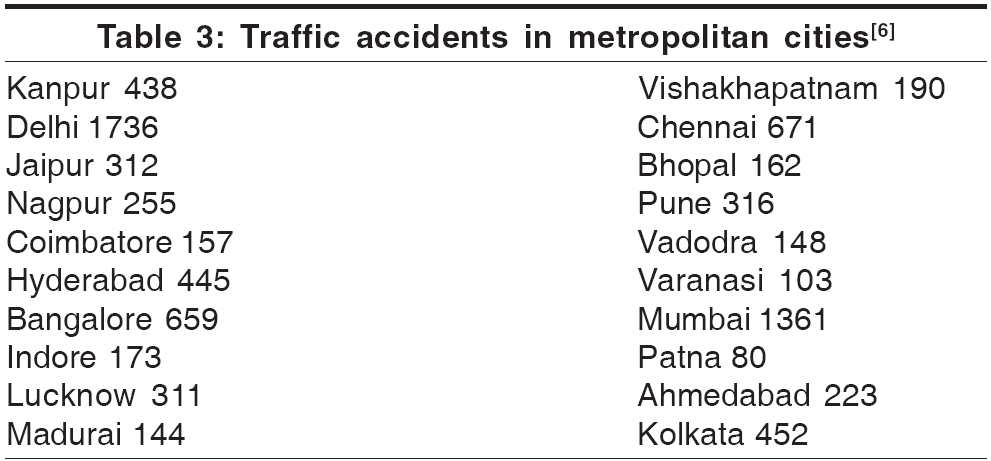
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 13-15 Special Article Synergy among the neuro-specialists Agarwal SP Director General of Health Services, Government of India, New Delhi Code Number: ni06002 Traditionally the burden of disease has been derived from mortality statistics. These data tend to ignore the burden associated with non-fatal conditions like mental and neurological disorders, which do not figure in the ′cause of death′ lists, but which, nevertheless, are associated with significant caregiver and societal costs. Over the past two decades, however, the underlying concepts have undergone significant changes. In accord with current thinking, disease burden measurement now includes time lived with disability and neuro-psychiatric disorders have come to be recognised as leading causes of the burden of disease worldwide [Table - 1]. With the progressive control of communicable diseases, specially in the third World countries, death rates have declined steeply and average life expectancy has risen, on an average, from 40 to 66 years. In contrast, mental and neurological problems, which affect hundreds of millions of people, have become major contributors to the global disease burden, as vividly illustrated by the following data [Table - 2]. Epilepsy alone constitutes a huge burden, with estimates ranging from 2-10 per 1000 population in the South East Asia Region (SEAR).[2] Studies from different parts of India reveal that prevalence varies between 9/1000 in Bangalore, 5/1000 in Mumbai and 4/1000 in New Delhi. Apart from the paucity of specialised medical services, the ignorance and stigma associated with many neurological disorders, such as epilepsy and dementia, constitute a major hurdle in the pathways to care. This holds good for mental disorders as well. Such prejudice contributed to the horrifying tragedy at Erwady in the Ramanathapuram district of Tamil Nadu where 26 chained mental patients got burnt alive in a "dargah" asylum fire during Aug 2001. This happened inspite of the fact that psychiatric facilities were available in the government district hospital located a mere 8 km away. This in itself constitutes a strong argument for seeking synergy between the neurosciences and mental health. Another area of concern is traumatic brain injury (TBI), which may well be termed a disease of development, related to the growth of civilization. It is a matter of grave concern for individuals, institutions and governments. It constitutes a major source of disability and distress not only for the patients, but also for the family and the society in terms of emotional burden, loss of work force and financial drain. It is an ongoing pandemic, with an annual incidence of two million cases per year in a developed country like the US.[3] During 2002, an estimated 1.18 million people worldwide died as a result of such injuries, i.e, 2.1% of the global morbidity due to all causes.[4] In the US, the costs related to such injuries are estimated at 1-2.5% of the gross domestic product (GDP). Translated to the Indian context, this would come to a mind-boggling sum, in terms of human resources as well as finances, which the country can ill afford. Road traffic accidents (RTAs) are the major contributor (60%) to TBIs and Indians roads are perhaps the most unsafe in the world: with just 1% of the world′s motor vehicles, the country accounts for 6% of the world-total of RTAs. In New Delhi alone there were nearly 20000 traffic accidents and over 2000 traffic-related fatalities during 2001-2002.[5] This is not surprising in view of the fact that the number of motor vehicles registered in India had gone up from 1.4 million in 1970 to 40 million in the year 2000 [Table - 3]. The incidence of head injuries is steadily rising in tandem with urbanization and the quantum increase in the number of vehicles on the roads. On an average 80,118 Indians are killed and over 342,200 suffer injuries every year in road traffic accidents, which is higher than in any other country in the world.[6] Alcohol contributes to about 15-20% of these injuries.[7] India and other developing countries face major challenges in the areas of prevention, pre-hospital care, specialised trauma centres and rehabilitation to reduce the burden of mortality and morbidity related to TBIs. Delhi itself presents a grim picture, with about 500 vehicles being added to its already clogged roads every day, while having one of the highest RTA rates in the world.[8] Many of these accident victims die before they reach hospitals with the requisite emergency trauma-care services. In order to reduce such avoidable mortality, a scheme has been formulated for providing financial assistance to state government hospitals located in cities and towns along the national highways for upgrading their emergency services. It envisages financial support to designated hospitals to cover the cost of well-equipped ambulances, resuscitative and other trauma-care services, communications systems, infrastructure facilities like X-ray, operation theatre and blood bank and essential medical equipment. It is hoped that a well organised network of emergency treatment, evacuation and trauma-care services will help reduce the mortality resulting from road traffic accidents. The recently enunciated National Health Policy - 2002 (NHP-2002), coming almost two decades after the previous 1983 policy, looks at a variety of issues in the health arena. It specifically envisages the establishment of fully equipped ′hub-spoke′trauma-care networks in large urban conglomerates in order to reduce accident-related mortality. The proposed National Highway Trauma Care Project is an innovative trauma care system, envisaged to cover the entire Golden Quadrilateral segment, connecting Delhi- Kolkata- Chennai- Mumbai and the North- South and East- West corridor. The project aims at establishing an integrated network, providing optimal of care for the trauma victims. This is expected to bring down the preventable deaths to 10% of the present level. In view of the relatively limited availability of neurosurgeons and neurologists, however, most of this care will be administrated by general: surgeons, physicians and medical officers. There is, therefore, a strong case for equipping these doctors with the necessary basic skills in order to ensure minimum standards of care. The NHP-2002 also envisages a network of decentralized mental health services for ameliorating the more common categories of neuro-psychiatric disorders. The budgetary support for the National Mental Health Programme (NMHP) has been increased nearly 7- fold, to Rs 1900 million in the 10th Five Year Plan, up from Rs 280 million when the project was initiated on a pilot basis during the 9th Plan. This quantum accretion in the resource base is being utilized as under:
Total: Rs. 1900 million The main thrust of the restrategised National Mental Health Programme is to provide community based mental health care, integrated with the existing general health care system, in 100 districts across the country in the first phase and 100 more in the second phase during the 10th Five Year Plan. The restrategised NMHP offers a potential vehicle for the provision of basic neurological / neurosurgical services on a hitherto unimaginable scale. If we could rise to the occasion and evolve community based treatment strategies, it may be possible to meet these specialised health needs of the people through the existing public health delivery system. As in the case of NMHP, it should be possible to equip general duty medical offers with skill-based training in basic neurological methods in order to ensure early recognition and effective management of common neurological disorders at the primary care level. A proposal to integrate the treatment for epilepsy and dementia with the District Mental Health Programme is under examination and it may be possible to achieve this without substantial additional budgetary support. Three salient facts emerge from the foregoing. The neuro-specialities, neurology, neurosurgery and psychiatry, have much in common. All three deal with the mind, albeit from different perspectives. The clinical approach is strikingly similar, as also the basic investigative aids, EEG, CT scan and MRI. There are significant commonalities in training, together with frequent overlap in diagnosis and management. This is, perhaps, best illustrated by common clinical conditions like headache, giddiness and seizure disorders. Also, in all three specialities, there is a gross mismatch between the availability of trained manpower and the huge magnitude of the disease burden, necessitating the delivery of specialised care through primary care physicians, who have been given the required skill-based training. In such a scenario, sharing of resources makes sound common sense. While there is a dedicated national programme for mental health, with adequate fiscal support, neurology and neurosurgery are less fortunate in this regard. Using the National Mental Health Programme infrastructure to extend neurological and neurosurgical services through the existing primary health care system, therefore, appears to be the most cost-effective strategy in our context. This will also ensure the optimum utilisation of the investigative facilities (EEG, ultrasound, CT Scan etc) provided to selected hospitals in 144 districts across the country, at a total cost of Rs 432 crore, as part of the 11th Finance Commission recommendations. The fraternity of neuro-scientists may deliberate on the above issues. The concept is not as utopian as it may sound at first. As stated earlier, the economics of the strategy have been worked out. It is perhaps the most cost-effective means of achieving the objective of decentralizing neurological care to the periphery and make it accessible to vast sections of our population, who would not otherwise ever reach neurology OPDs. The first step needs to be taken at the apex. The leading experts of neurology, neurosurgery and psychiatry should come together in this search of synergy. I have no doubt that this would be a seminal association. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06002t1.jpg] [ni06002t3.jpg] [ni06002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}