
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 54, Num. 1, 2006, pp. 16-23
|
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 16-23
Review Article
Medulloblastomas: New directions in risk stratification
Sarkar Chitra, Deb Prabal, Sharma MeharChand
Department of Pathology, All India Institute of Medical Sciences, New Delhi
Correspondence Address:Department of Pathology, All India Institute
of Medical Sciences, Ansari Nagar, New Delhi - 110 029, drchitrasarkar@yahoo.com
Code Number: ni06003
Abstract
Medulloblastomas (MBs) are the most common malignant brain tumors in children. Current therapeutic approaches combine surgery, radiotherapy, and chemotherapy. Although, there has been significant improvement in long-term survival rates, the tumor remains incurable in about a third of patients while cognitive deficits and other sequelae of therapy are common among long-term survivors. Hence a major challenge remains to differentiate high-from low-risk patients and to tailor therapy based on the degree of biological aggressiveness. A clinical risk-stratification system has been widely used in MBs based on age, extent of resection and the Chang staging system. However, recent reports indicate that these clinical variables are inadequate methods of defining disease risk. This has prompted search for new markers for MB stratification. Recent studies indicate that the classification of MBs according to profiles of histopathology and molecular abnormalities possibly help better risk-stratification of patients, thereby rationalizing approaches to therapy, increasing cure rate, reducing long-term side effects and developing novel therapeutic strategies. The most accurate outcome prediction till date has been obtained through microarray gene expression profiling. In this article, the current histopathological classification and the recent advances in molecular genetics of MBs are reviewed. Global efforts to translate this knowledge of disease biology into clinical practice especially as outcome predictors are highlighted.
Keywords: Histopathology, medulloblastoma, molecular genetics,
prognostic factors, risk-stratification.
Medulloblastoma (MB) is one of the five embryonal tumors of the central nervous system (CNS) included in the current WHO classification (WHO Grade IV).[1] It is a highly malignant tumor of the cerebellum occurring predominantly in children and accounting for 12-25% of all pediatric CNS tumors.[2],[3],[4],[5],[6] It is less frequent in adults, constituting only 0.5-1% of all intracranial neoplasms.[7],[8],[9],[10],[11]
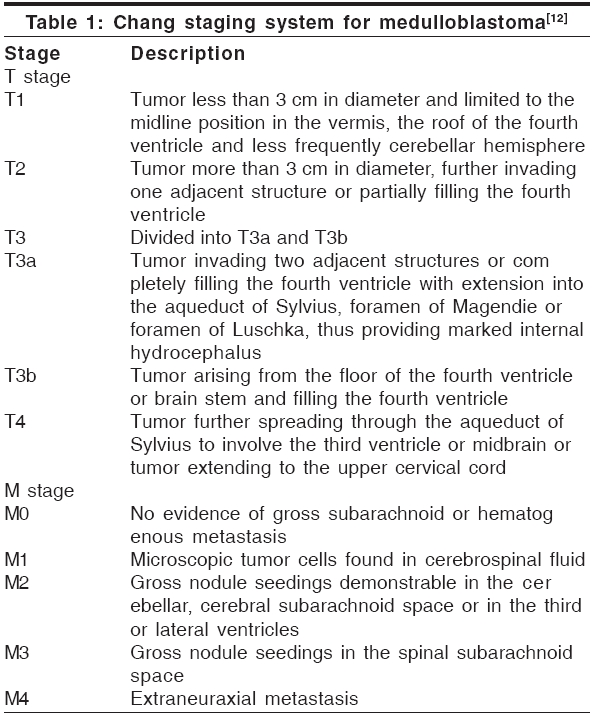
A. Risk stratification by clinical factors
Since the mid-1990s, the risk classification for relapse and selection
of treatment of MB patients has remained strictly clinical, with cases
stratified into two-risk groups, viz. ′average risk′ and ′high risk,′based
on the following criteria: (i) age, (ii) extent of resection, and (iii)
Chang metastasis staging [Table - 1].[12],[13]
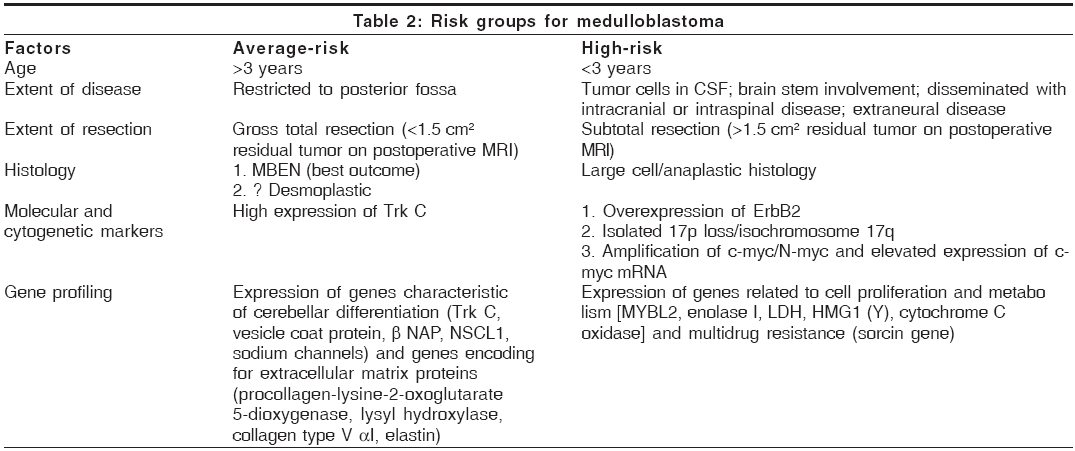
According to this classification, average-risk patients are those
older than 3 years of age with nonmetastatic disease and totally or near
totally resected tumors (< 1.5 cm of residual tumor on postoperative
MR). Patients not fulfilling these criteria are regarded as high-risk . This clinical staging has been helpful as a broad guide for predicting prognosis. However a major drawback is that this does not differentiate high- from low-risk patients within the same clinical stage. It is a well-observed fact that patients with similar neoplasms and similar clinical stage, receiving identical therapies can have widely disparate clinical outcomes, owing to biological differences within the tumor.[14] Further,
two different trials, German trial HIT′91 and CCG 921[13],[15] have established that overall survival (OS) is not significantly different between children staged as M0 vs those staged as M1. Also, brain stem invasion (stage III b), previously regarded as an indicator of high-risk, is now believed not to affect prognosis.[13]
Based on this clinical staging system, a multimodality therapeutic approach has been designed for MBs, with maximum surgical resection, neuraxis radiation and chemotherapy.[16] This
has led to a reduction in the mortality rate by twofold in the last 30
years, with OS rates ranging from 50 to 60% at 5 years and 40-50% at
10 years.[17] However, in long-term survivors of MBs, this aggressive protocol is associated with severe side effects in the form of neuropsychological sequelae and neurocognitive decline.[18],[19].[20],[21]
In short, the major criticism of the current clinical staging is that
it does not identify the 20-30% of average-risk patient with resistant disease or the average-risk patients who might be over treated with the current protocol.[18] Hence, an important goal is to improve the chances of survival for all children with MB, and to tailor specific therapies to individual lesions based both on their degree of clinical as well as biological risk, so that patients are not over- or under-treated, and side effects are minimized.
All this has prompted search for new biological markers - histological
and molecular - for MB stratification. It is hoped that a greater understanding
of MB biology will not only translate into refinements in risk classification,
but also lead to risk-based tailoring of therapies to individuals. It
will also help in improvements in the way existing therapies are used,
which is crucial in minimizing their devastating long-term side effects.
B. Risk stratification by histopathological factors
Recent studies have conclusively demonstrated that the following
three histological factors have a distinct role in the determination
of clinical outcome in MB viz. histopathological subtype, extent of nodularity
and grade, as well as, extent of anaplasia [Table - 2]. The other factors
implicated to have prognostic significance include desmoplasia, cell
differentiation, proliferation, apoptosis, and ploidy. However, their
definite role still remains controversial.
1. Histopathological subtypes
Six distinct histological subtypes of MB have been included
in the current WHO classification.[4]
Classic MBs are characterized by sheets of densely packed cells with
hyperchromatic small round to oval nuclei, indiscernible cytoplasm, numerous
mitoses, conspicuous apoptosis, and formation of occasional Homer Wright/neuroblastic
rosettes.[4],[22],[23]
Desmoplastic MBs, on the other hand, show typical nodular architecture
comprising of reticulin-free pale nodules and reticulin-rich internodular
regions.[4],[22],[23]
Medulloblastomas with extensive nodularity and advanced neuronal differentiation
(MBEN) are a distinct subtype, occurring in infants less than 3 years
of age and demonstrating a striking grape-like nodularity on imaging.[24] Histologically,
they show a predominant nodular architecture with round uniform cells
inside nodules arranged in a streaming pattern within a fine fibrillary
neuropil-like matrix. Thus they differ from desmoplastic MBs in showing
uniform neurocytic differentiation with little or no internodular component.[4],[22],[23]
LC/A MBs comprise of large cells with pleomorphic nuclei, prominent nucleoli
and more abundant cytoplasm than most MBs. High mitotic and apoptotic
rate along with large areas of necrosis are also common.[4],[22],[23],[25]
Melanotic MBs, are characterized by melanin production in scattered cells,[26],[27] while
medullomyoblastomas consist of cells displaying variable rhabdomyoblastic
differentiation,[28],[29],[30],[31] both
in a background of classic MB.
Of all the six variants the best prognostic outcome is noted with MBENs.[24],[32] This
is intriguing because it generally affects young infants who according
to the clinical stage belong to the high-risk category. The worst outcome
is associated with LC/A MBs, which are extremely aggressive with high
incidence of local recurrence, CSF spread, systemic metastasis and death
within 1-2 years of diagnosis.[25],[33]
Difference in prognosis between the classic and desmoplastic variants
remains controversial. Desmoplastic MBs have been variably correlated
with better outcome[34],[35],[36] by
some, while others found it to be either associated with worse prognosis,[37] or
without any correlation with survival time.[9],[38],[39]
Melanotic MBs and medullomyoblastomas have poor outcome, with survival
ranging from 2 months to 2.5 years, in the former, and generally less
than 1 year, in the latter subtype.[26],[29]
2. Extent of nodularity
Eberhart et al[38] demonstrated
nodularity in 29% of 330 similarly treated cases of pediatric MB from the Pediatric Oncology Group (POG, USA). However, nodule formation in MBs can be variable - from diffuse to very focal. Hence, they graded the extent of nodularity into five categories - extensive (96-100%), widespread (51-95%), moderate (11-50%), slight (1-10%), and none (0%),
and observed that only tumors with extensive nodules were associated with
better survival. All other grades of nodularity showed no correlation with
outcome.[38]
3. Anaplasia
The concept of anaplasia in MBs is relatively new[14] and
analogous to anaplasia in Wilm′s tumor, which has well defined clinical
implications.[40] Anaplastic
MBs have currently been proposed as the variant with most aggressive biological
behavior.
Anaplastic MBs are characterized by markedly atypical cells having
angular pleomorphic nuclei with coarse chromatin, wrapping around each
other, with
frequent moulding.[14],[38],[41],[42] Earlier
studies suggested that anaplasia was only confined to the large cell variant
of MB. However, recent studies have shown that they can also arise by malignant
progression of classic and desmoplastic MBs, as well as medullomyoblastomas.[14],[42],[43] These
cells are thought to represent focally aggressive clones capable of undergoing
malignant progression, based on the observation that they often co-exist
focally within MBs, or manifest only after recurrence or metastasis.[14],[43],[44],[45]
Brown et al[41] in a review
of 474 MBs from POG patients, reported that the long-term survival of LC-MB
with anaplasia was 10% compared to more than 50% in LC-MB
without anaplasia. Eberhart et al[38] on
reevaluating 330 of the POG patients reported by Brown et al[41] observed
that while tumors with diffuse anaplasia were most aggressive, even focal
anaplasia was significantly associated with poor outcome. Further patients
with tumors having moderate to severe anaplasia (anaplastic group) had
significantly shorter event-free survival (EFS) and OS as compared to those
with slight to no anaplasia (nonanaplastic group). The 5-year survival
probability was 42% inpatients with anaplastic variant in contrast to 68% for
patients with nonanaplastic disease. In fact, on log-rank analysis, grade
of anaplasia allowed better stratification of patients with respect to
outcome than the current clinical stage, indicating that histological grading
is not a surrogate for clinical staging, but rather an independent predictor
of survival. Similar results of association of anaplasia with poor outcome
have also been shown by MacManamy et al.[33]
4. Desmoplasia
Conflicting reports on relationship of desmoplasia to outcome are chiefly
attributable to different definitions of desmoplasia.[42] In
addition to conventional desmoplastic MBs, rarely MBs show an intense pericellular
desmoplasia without any obvious nodule formation. Further invasion of leptomeninges
by classic MB also produces intense desmoplasia.[42]
In a retrospective review of 330 POG patients, Eberhart et al[38] noted
desmoplasia in 22% of cases. However there was no significant association
of desmoplasia with clinical outcome (either EFS or OS).
5. Cell differentiation
Another histopathological prognostic parameter in MBs, which has received
considerable attention but little agreement, is differentiation along glial
or neuronal cell lines.[46] Positivity
for GFAP have been variably correlated with better prognosis[47],[48] by
some, while others found it to be either associated with poor prognosis,[49],[50] or
without any correlation with survival time.[51],[52]
6. Proliferation/labeling index (LI)
Cell proliferation is another prognostic parameter whose significance
is not clear. Ito et al[53] showed
that tumors with Bromodeoxyuridine (BudR) LI greater than 20% had
a trend to worse prognosis. In contrast, Giordana et al[37] and
Schiffer et al[54] showed
no correlation in both adult and pediatric MBs. Studies of Sarkar et al[6] suggested
that MBs in children have higher MIB-I proliferative indices and lower
apoptotic indices than those in adults.
7. Apoptotic index (AI)
Since it is the balance between cell proliferation and cell death that
determines the rate of tumor growth, the impact of apoptosis on outcome
has also been considered. Apoptosis has been suggested as a favorable prognostic
feature by some[55] and as
a negative feature by others.[56],[57] Korshunov
et al[57] calculated
AI of> 1.5% to be associated with shorter survival, while Eggert
et al[58] found that expression
of Apo3 was significantly associated with prolonged survival of MB patients.
Haslam et al[55] demonstrated
that patients with a high AI had substantially improved outcome compared
to all other patients, independently from the assignment to a high- or
low-risk group at the time of diagnosis.
8. Ploidy
A more favorable prognosis has been associated with aneuploidy in MBs.
Ramachandran et al[59] found
that patients with aneuploid tumors responded well to treatment regimens
as compared to those with diploid tumors. Also, patients with progressive
disease had a high S-phase fraction in the tumor cell population as compared
with patients with favorable response to treatment.
C. Risk stratification by molecular and cytogenetic factors
It is widely accepted that identification of genetic and molecular
alterations allows a clinically relevant subgrouping of MBs with particular
profiles of biological behavior and outcome [Table - 2]. [60],[61],[62],[63],[64],[65],[66] The
molecular genetic alterations in MBs have been worked out extensively and
can be divided into three heads:
- Nonrandom chromosomal abnormalities,
- Gene profiling,
- Abnormalities in signal transduction pathways.
1. Nonrandom chromosomal abnormalities
(i) Loss of 17p/isochromosome 17q
The most frequent genetic alteration present in 30-50% of
MB cases is partial or complete deletion of the short arm of chromosome
17
(17p), [67],[68],[69],[70],[71] which
may occur in isolation, but more frequently as a component of an isochromosome
of 17q [i(17q)].[69],[72],[73],[74] A
recent study suggested that 17p loss /isochromosome 17q is more frequent
in LC/A MBs than in classic MBs.[14]
Several authors have observed that 17p deletion and/or i(17q) are prognostically
unfavorable being associated with poor response to therapy, metastatic
disease and shortened survival.[75],[76] However,
other studies have refuted this suggestion.[72],[77] Scheurlen
et al[76] reported that MBs
with concomitant 17p alterations and c-myc alterations have worse
prognosis, indicating possible interaction between these two genetic alterations
in promoting aggressive behavior.
Mutations of the tumor suppressor gene, p53 , located at 17p13.1
region are infrequent in MBs.[78],[79] However,
an association of intense p53 immunostaining with significant reduced disease-free
survival in MB patients has been shown by Woodburn et al[80] Similarly,
hypermethylation of the HIC-1 gene, on 17p13.3 region has been
demonstrated to be a predictor of poor outcome in MB.[81]
(ii) Myc gene (c-myc and N-myc) amplification
Amplification of c-myc and/or N-myc occurs in 5-10% of
MBs, being most commonly associated with the LC/A variant.[45],[82],[83],[84],[85],[86],[87] Eberhart
et al[45] found amplification
of c-myc in
4 (12%) and N-myc in 5 (15%) of 33 MBs, all with
anaplastic foci. A very high rate of c-myc amplification of 17% was
reported by Scheurlen et al[76] among
a population of clinically high-risk MBs.
There is clear evidence that patients whose tumors show c - myc gene
amplification have worse clinical outcome, being resistant to therapy and
having an aggressive course with short survival and fatal outcome. Aldosari
et al[82] found 4 of 77 MBs
with c-myc amplification
(5.2%) all of whom died within 7 months of diagnosis. One case having
amplification for both c-myc and N-myc and four cases with
only N-myc amplification were also associated with short survival
time. In the series of Badiali et al[84] no
long-term survivors were observed among cases with c-myc amplification.
Similarly Scheurlen et al[76] showed
that all tumors with c-myc amplification were resistant to therapy
and had fatal outcome.
A similar negative correlation of outcome with c-myc mRNA levels was
shown by Herms et al[87] and
Grotzer et al[88] Around
42% of MBs showed c-myc mRNA expression, and this parameter was
found to be an independent prognostic criteria and more predictive than
standard clinical factors.[87]
High rate of immunopositivity for both c-myc protein (90%)[89] and
N-myc protein (84%)[90] have
also been reported in MBs. A tendency of N-myc immunopositive MBs to be
associated with poor outcome was shown by Moriuchi et al.[90] Hence
there is a need of identifying MBs with myc gene amplification or myc mRNA
over expression, since a large body of evidence now indicates its association
with aggressive clinical behavior.
(iii) Other chromosomal abnormalities
In 20-40% of MB cases, loss of chromosomes 1q and 10q has been
demonstrated.[91],[92] Isolated
examples of deletions of 3q, 6q, 9q, 10q, 11p, 11q, and 16q as well as
gains of distal regions of 4p, 5p, 5q, 7q, 8q, and 9p have also been detected
in MBs.[83],[93],[94] However,
till date no prognostic correlation has been attached to any of these chromosomal
abnormalities, with the exception of 9q loss (locus of PTCH Gene).
Lusher et al[95] has reported
inactivation of the RASSF-1A gene
on chromosome 3p21 in 79% of MBs (both in adult and pediatric MBs
and in all histological variants).
Recently, Tong et al[96] performed
the first genomic survey of multiple oncogenes amplifications involved
in the development of MBs. For the first time they identified gene amplifications
involving PGY1 at 7q21.1, MDM2 at 12q14.3-q15, and Erb2
at 17q21.2, by performing comparative genomic hybridization (CGH) and array-based
CGH, in a series of 14 cases. Overall the highest frequency of oncogene
gains was observed in D17S1670 (61.5%), PIK3CA (46.2%), PGY1 (38.5%), MET (38.5%),
and CSE1L (38.5%). Gene amplification in MBs was further
confirmed by using fluorescence in-situ hybridization (FISH) analysis in
34 additional archival MB cases. In future, gains in these genes may possibly
qualify as candidates for molecular markers and therapeutic targets of
MBs.
2. Gene profiling
Pomeroy et al[97] studied
gene expression profile of MB cases using oligonucleotide microarrays.
The genes most closely correlated with MBs were ZIC and NSCL1 ,
which encode transcription factors specific to cerebellar granule cells.
They also identified a number of genes, which correlated with favorable
outcome, including many genes characteristic of cerebellar differentiation
( vesicle coat protein β-NAP, NSCL1, TrkC, sodium channels ), and
genes encoding extracellular matrix proteins ( procollagen-lysine-2-oxoglutarate 5-dioxygenase, lysyl hydroxylase, collagen type V α-I, elastin ).
In contrast, genes related to cerebellar differentiation were underexpressed
in poor prognosis tumors, which were dominated by the expression of genes
related to cell proliferation and metabolism [ MYBL2, enolase I, LDH, HMG1 (Y), cytochrome C oxidase ]
and multidrug resistance ( sorcin gene ).
Their study further demonstrated that outcome predictions based on
gene expression (with a model made up of eight genes) was statistically
significant:
patients with a certain pattern, expected to have a good prognosis, had
a 5-year OS of 80% compared with 17% for those not having
that pattern, for whom a poor outcome was predicted.
In another study of gene expression profiles, MacDonald et al[98] described
that the platelet derived growth factor receptor alpha (PDGFR-α) and the
Ras/mitogen-activated protein (MAP) kinase pathway genes were significantly
upregulated in metastatic (M+) tumors but not in nonmetastatic (M0) MBs, This finding suggests that the PDGFR-α and Ras/MAP kinase signal transduction pathway may be rational therapeutic targets for M+ disease.
3. Abnormalities in signal transduction pathways
(i) Neurotrophin signaling pathway - TrkC expression and outcome
This pathway plays a major role in cerebellar development. It comprises
of the neurotrophin family, which includes a set of ligands viz. nerve
growth factor (NGF), brain derived neurotrophic factor (BDNF), neurotrophin
factors 3, 4, and 5 (NT3 and NT4/5). These are essentially trophic factors
for the growth differentiation, survival and apoptosis of neurons. The
other major constituent of this pathway are three members of the tyrosine
kinase receptor family viz. TrkA, B, C. These Trk proteins function as
classical growth factor receptors, each binding to one of the four neurotrophins
resulting in their activation and upregulation of second messenger signaling
pathway systems.[99],[100],[101]
TrkC expression has been reported in 48-85% of MBs in different
series.[102],[103] This
high TrkC expression has been found to be the single most powerful independent
predictor of favorable outcome in MBs, independent of other clinico-pathological
variants. It was Segal et al[104] who
first reported 5-year survival rates as high as 89%, in patients having tumors with high TrkC expression, as compared to 46% for
those with low TrkC expression levels. Subsequently Kim et al[105] in
a study of 42 cases of MB found that the median survival in high expressers
of TrkC was 92 months, in contrast to only 39 months for the low expressers.
In a larger study of 81 MBs and 6 PNETs, Grotzer et al[106] reported
a 4.8-fold greater risk of death in children with tumors having low TrkC
mRNA expression. They identified TrkC mRNA expression as a powerful independent
prognostic factor for predicting progression-free and OS. In another study,[88] they
showed 100% progression-free survival in a group of PNET/MB patients
having combined low c-myc and high TrkC mRNA expression in their tumors
after a median follow up time of 55 months. Contradictory results have
been reported by Gajjar et al[18] who
found no correlation of TrkC expression with clinical outcome.
(ii) ErbB receptor signaling pathway - ErbB2 expression and outcome
The class-I receptor tyrosine kinases (RTK1), also termed ErbB/HER
receptors constitute a signal transduction pathway that is important in
both cerebellar development and MB tumorigenesis.[107],[108] Of
the four members of this family viz. ErbB1, B2, B3, and B4, Erb B2 receptor
appears to play a central role in MB tumorigenesis, along with neuregulin-1b
(NRG-1b). ErbB2 expression has been reported in> 80% of MBs, with co-expression of ErbB4 in 54% and expression of NRG-1b in 87.5% of
tumors.[62],[107],[109],[110],[111] However,
Gajjar et al[18] found
ErbB2 expression in only 40% of tumors, most frequently in the LC/A
variant.
Association between reduced patient survival and increased ErbB2 expression
has been demonstrated by several workers.[18],[62],[110],[111],[112] Gilbertson
et al[110] first
reported a 48% 10-year survival rate in cases with less than 50% ErbB2-positive tumor cells, while the corresponding figures for cases ≥ 50% positive cells was 10%. This prognostic significance was maintained in a further extension of the study to 70 cases, with 25-year survival rates for cases with < 50% and ≥ 50 ErbB2 expression being 46 and 17%,
respectively.[111] In the
same study, they[111] also
showed that co-expression of ErbB2 and ErbB4 significantly correlated with
reduced OS, being independent of other clinical variables like age and
tumor stage. Further, co-expression of all three components viz. ErbB2,
ErbB4, and NRG-1b was significantly associated with presence of CNS metastasis
at diagnosis.[107]
It has been shown that combined analysis of molecular and clinical factors
gives better risk stratification than clinical factors alone. Thus in an
analysis of 41 MBs, Gilbertson et al[62] found
that sub-total tumor resection, metastatic disease at diagnosis, high expression
of ErbB2 and isolated 17 p loss, all negatively correlated with survival.
Similarly Gajjar et al[18] in
a study of clinical average-risk childhood MBs reported 100% 5-year survival in ErbB2-negative disease cases, as compared to only 54% in
ErbB2-positive tumors.
(iii) Hedgehog - (SHH/PTCH) signaling pathway
Sonic hedgehog (SHH), the principal member of the hedgehog pathway,
is a family of ligands, which are involved in cerebellar development by
promoting replication of granule cells.[113] PTCH (patched)
is a tumor suppressor gene located on 9q22.3, which encodes a trans-membrane
PTCH protein product. This is activated by SHH and functions as part of
a signaling pathway controlling normal CNS development.[114],[115],[116] The
SHH/PTCH pathway has been implicated in the development of both sporadic
and heritable forms of MB. Mutations in several components of the SHH pathway
occur in about 25% of sporadic MB cases, commonest being mutation
of the PTCH gene, reported in 8-12% of tumors.[117],[118],[119] In
patients with Gorlin′s syndrome or NBCCS who have germ-line mutations
of the PTCH gene the lifetime risk of developing MB is about 4%.[114],[116],[120] It
has been observed that MBs that carry mutations in the SHH/PTCH pathway
preferentially but not exclusively show nodular desmoplastic morphology.[121],[122] However,
till date no association has been found of alterations in this signaling
pathway with prognosis in MBs.
(i) Wingless (WNT/WG) pathway
The WNT pathway co-ordinates a diverse array of developmental processes
including the proliferation and fate of neural progenitor cells.[122],[123] The
components of this pathway include β-catenin, the key transcriptional activator
which in turn associates in the cytoplasm with a complex, which includes
adenomatous polyposis coli ( APC ) gene, glycogen synthase kinase-3
(GSK3β) and AXIN-1.[122],[123]
Mutations in proteins of the WNT pathway, especially of β-catenin and APC gene
occur in about 15% of sporadic MBs. [124],[125],[126],[127],[128] Mutations
of APC gene
are also the cause of Turcot′s syndrome, a tumor predisposition
syndrome characterized by development of bowel tumors and MB.[129]
No correlation again has been found with this pathway and prognosis. However
an increasing number of anti-cancer drugs are being designed to target
this pathway. Cyclopamine, is one example of a plant-derived teratogen,
that specifically inhibits the SHH pathway in MB cells, causing anti-tumor
activity.[130] Conclusion
There has been marked improvement in the 5-year survival rates in MBs
from 2-30% in the 1970s to 50-70% currently. A major challenge, however, remains to differentiate high- and low-risk patients, and to individualize patient therapies, so as to prevent long-term side effects. In this regard, clinical staging alone has been shown in various studies to have its limitations. Two histological parameters currently assuming prognostic importance in MBs are the histopathological variant and grading of anaplasia. It is becoming apparent that homogenous lumping of all MBs as grade IV, highly aggressive neoplasms may be unjustified. The new concept therefore is to categorize MBs into favorable versus unfavorable histological groups, which is comparable to the classification used for peripheral neuroblastomas and Wilms′tumors.
Molecular prognostic markers also hold promise, though global, multi-institutional
studies with larger number of patients are required to prospectively
validate their role as well as the methodologies used for the assessment
of their expression levels.
The detailed mechanisms of how the different
signaling pathways mediate an oncogenic effect need to be identified
if we are to exploit these pathways fully for patient prognostication
and management. Further, several questions need to be answered -which
pathways initiate MB formation and which are involved in disease progression;
how specific pathways affect MB histopathology and behavior; and whether
any signal pathways mediate resistance to conventional treatments.
It is possible that in such a complex interaction of several factors,
a final scenario will emerge where in a combination of clinical,
histopathological and molecular factors will provide a more reliable
means of disease
stratification in patients of MB, rather than any single parameter
alone. The role of the Pathologist will then assume great importance
in guiding clinicians regarding biological risk assessment and tailoring
therapeutic strategies.
References
| 1. | Kleihues P, Cavenee WK (editors). World Health Organization Classification of Tumours, Pathology and Genetics of Tumours of the Nervous System. Lyon, France: IARC Press; 2000. p. 6-7. Back to cited text no. 1 |
| 2. | Arseni C, Ciurea AV. Statistical survey of 276 cases of medulloblastoma (1935-1978). Acta Neurchir (Wien) 1981;57:159-62. Back to cited text no. 2 [PUBMED] |
| 3. | Farwell JR, Dohrmann GJ, Flannery JT. Medulloblastoma in childhood: an epidemiological study. J Neurosurg 1984;61:657-64. Back to cited text no. 3 [PUBMED] |
| 4. | Giangaspero F, Bigner SH, Kleihues P, Pietsch T, Trojanowski JO. Medulloblastoma. In: Kleihues P, Cavenee WK (editors). World Health Organization Classification of Tumours, Pathology and Genetics of Tumours of the Nervous System. Lyon, France: IARC Press; 2000. p. 129-37. Back to cited text no. 4 |
| 5. | Roberts RO, Lynch CF, Jones MP, Hart MN. Medulloblastoma: a population-based study of 532 cases. J Neuropathol Exp Neurol 1991;50:134-44. Back to cited text no. 5 [PUBMED] |
| 6. | Sarkar C, Pramanik P, Karak AK, Mukhopadhyay P, Sharma MC, Singh VP, et al. Are childhood and adult medulloblastomas different? A comparative study of clinicopathological features, proliferation index and apoptotic index. J Neurooncol 2002;59:49-61. Back to cited text no. 6 [PUBMED] [FULLTEXT] |
| 7. | Ferrante L, Mastronardi L, Celli P, Acqui M, Cervoni L, Fortuna A. Medulloblastoma in adulthood. J Neurosurg Sci 1991;35:23-30. Back to cited text no. 7 [PUBMED] |
| 8. | Giordana MT, Schiffer P, Lanotte M, Girardi P, Chio A. Epidemiology of adult medulloblastomas. Int J Cancer 1999;80:689-92. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Hubbard JL, Scheithauer BW, Kispert DB, Carpenter SM, Wick MR, Laws ER. Adult cerebellar medulloblastomas: the pathological, radiographic and clinical disease spectrum. J Neurosurg 1989;70:536-44. Back to cited text no. 9 |
| 10. | Muleci A, Cervoni L, Delfini R. Medulloblastomas in children and in adults:a comparative study. Acta Neurochir (Wien) 1992;119:62-7. Back to cited text no. 10 |
| 11. | Pramanik P, Sharma MC, Mukhopadhyay P, Singh VP, Sarkar C. A comparative study of classical vs. desmoplastic medulloblastomas. Neurol India 2003;51:27-34. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | Chang CH, Housepian EM, Herbert C. An operative staging system and a megavoltage radiotherpeutic technic for cerebellar medulloblastoma. Radiology 1969;93:1351-69. Back to cited text no. 12 |
| 13. | Zeltzer PM, Boyett JM, Finlay JL, Albright AL, Rorke LB, Milstein JM, et al. Metastasis stage, adjuvant treatment, and residual tumor are prognostic factors for medulloblastoma in children:Conclusions from the Children's Cancer Group 921 randomized phase II study. J Clin Oncol 1999;17:832-45. Back to cited text no. 13 |
| 14. | Eberhart CG, Burger PC. Anaplasia and grading in medulloblastomas. Brain Pathol 2003;13:376-85. Back to cited text no. 14 [PUBMED] |
| 15. | Kortmann RD, Kuhl J, Timmerman B, Mittler U, Urban C, Budach V, et al. Postoperative neoadjuvant chemotherapy before radiotherapy as compared to immediate radiotherapy followed by maintenance chemotherapy in the treatment of medulloblastoma in childhood: Results of the German prospective randomized trial HIT'91. Int J Radit Oncol Biol Phys 2000;46:269-79. Back to cited text no. 15 |
| 16. | Saran F. Recent advances in paediatric neuro-oncology. Curr Opin Neurol 2002;15:671-7. Back to cited text no. 16 [PUBMED] [FULLTEXT] |
| 17. | Brandes AA, Palmisano V, Monfardini S. Medulloblastoma in adults: clinical characteristics and treatment. Cancer Treat Rev 1999;25:3-12. Back to cited text no. 17 [PUBMED] [FULLTEXT] |
| 18. | Gajjar A, Hernan R, Kocak M, Fuller C, Lee Y, McKinnon PJ, et al. Clinical, histopathologic, and molecular markers of prognosis: toward a new disease risk stratification system for medulloblastoma. J Clin Oncol 2004;22:984-93. Back to cited text no. 18 |
| 19. | Heikens J, Michiels EM, Behrendt H, Endert E, Bakker PJ, Fliers E. Long-term neuro-endocrine sequelae after treatment for childhood medulloblastoma. Eur J Cancer 1998;34:1592-7. Back to cited text no. 19 [PUBMED] [FULLTEXT] |
| 20. | Walter AW, Mulhern RK, Gajjar A, Heideman RL, Reardon D, Sanford RA, et al. Survival and neurodevelopmental outcome of young children with medulloblastoma at St Jude Children's Research Hospital. J Clin Oncol 1999;17:3720-8. Back to cited text no. 20 |
| 21. | Mulhern RK, Palmer SL, Reddick WE, Glass JO, Kun LE, Taylor J, et al. Risks of young age for selected neurocognitive deficits in medulloblastoma are associated with white matter loss. J Clin Oncol 2001;19:472-9. Back to cited text no. 21 |
| 22. | Ironside JW, Moss TH, Louis DN, Lowe JS, Weller RO (editors). Embryonal tumours. In : Diagnostic pathology of nervous system tumours. London: Churchill Livingstone; 2002. p. 185-215. Back to cited text no. 22 |
| 23. | Burger PC, Scheithauer BW, Vogel FS. Surgical Pathology of the Central Nervous System and Its Coverings, 4th edn. Philadelphia: Churchill Livingstone; 2002. p. 298-338. Back to cited text no. 23 |
| 24. | Giangaspero F, Perilongo G, Fondelli MP, Brisigotti M, Carollo C, Burnelli R, et al. Medulloblastoma with extensive nodularity: a variant with favorable prognosis. J Neurosurg 1999;91:971-7. Back to cited text no. 24 |
| 25. | Giangaspero F, Rigobello L, Badiali M, Loda M, Andreini L, Basso G, et al. Large-cell medulloblastomas. A distinct variant with highly aggressive behavior. Am J Surg Pathol 1992;16:687-93. Back to cited text no. 25 [PUBMED] |
| 26. | Kalimo H, Haapasalo H. Melanotic medulloblastoma. In : Kleihues P, Cavenee WK (editors). World Health Organization Classification of Tumours, Pathology and Genetics of Tumours of the Nervous System. Lyon, France: IARC Press; 2000. p. 140. Back to cited text no. 26 |
| 27. | Sharma MC, Agarwal M, Suri A, Gaikwad S, Mukhopadhyay P, Sarkar C. A melanotic desmoplastic medulloblastoma: report of a rare case and review of the literature. Brain Tumor Pathol 2002;19:93-6. Back to cited text no. 27 [PUBMED] |
| 28. | Chowdhury C, Roy S, Mahapatra AK, Bhatia R. Medullomyoblastoma. A teratoma. Cancer 1985;55:1495-500. Back to cited text no. 28 [PUBMED] |
| 29. | Giordana MT, Wiestler OD. Medullomyoblastoma. In : Kleihues P, Cavenee WK (editors). World Health Organization Classification of Tumours, Pathology and Genetics of Tumours of the Nervous System. Lyon, France: IARC Press; 2000. p. 138-9. Back to cited text no. 29 |
| 30. | Lata M, Mahapatra AK, Sarkar C, Roy S. Medullomyoblastoma. A case report. Indian J Cancer 1989;26:240-6. Back to cited text no. 30 |
| 31. | Mahapatra AK, Sinha AK, Sharma MC. Medullomyoblastoma. A rare cerebellar tumour in children. Childs Nerv Syst 1998;14:312-6. Back to cited text no. 31 [PUBMED] [FULLTEXT] |
| 32. | Suresh TN, Santosh V, Yasha TC, Anandh B, Mohanty A, Indiradevi B, et al. Medulloblastoma with extensive nodularity: a variant occurring in the very young-clinicopathological and immunohistochemical study of four cases. Childs Nerv Syst 2004;20:55-60. Back to cited text no. 32 [PUBMED] [FULLTEXT] |
| 33. | MacManamy CS, Lamont JM, Taylor RE, Cole M, Pearson AD, Clifford SC, et al. Morphophenotypic variation predicts clinical behaviour in childhood non-desmoplastic medulloblastomas. J Neuropathol Exp Neurol 2003;62:627-32. Back to cited text no. 33 |
| 34. | Bailey CC, Gnekow A, Wellek S, Jones M, Round C, Brown J, et al. Prospective randomised trial of chemotherapy given before radiotherapy in childhood medulloblastoma. International Society of Paediatric Oncology (SIOP) and the (German) Society of Paediatric Oncology (GPO): SIOP II. Med Pediatr Oncol 1995;25:166-78. Back to cited text no. 34 [PUBMED] |
| 35. | Chatty EM, Earle KM. Medulloblastoma. A report of 201 cases with emphasis on the relationship of histological variants to survival. Cancer 1971;28:977-83. Back to cited text no. 35 [PUBMED] |
| 36. | Jenkin D, Shabanah MA, Shail EA, Gray A, Hassounah M, Khafaga Y, et al. Prognostic factors for medulloblastoma. Int J Radiat Oncol Biol Phys 2000;47:573-84. Back to cited text no. 36 [PUBMED] [FULLTEXT] |
| 37. | Giordana MT, Cavalla P, Chio A, Marino S, Soffietti R, Vigliani MC, et al. Prognostic factors in adult medulloblastoma. A clinico-pathologic study Tumori 1995;81:338-46. Back to cited text no. 37 [PUBMED] |
| 38. | Eberhart CG, Kepner JL, Goldthwaite PT, Kun LE, Duffner PK, Friedman HS, et al. Histopathologic grading of medulloblastomas: a Pediatric Oncology Group study. Cancer 2002;94:552-60. Back to cited text no. 38 [PUBMED] |
| 39. | Garton GR, Schomberger PJ, Scheithauer BW, Shaw EG, Ilstrup DM, Blackwell CR, et al. Medulloblastoma: Prognostic factors and outcome of treatment:review of the Mayo Clinic experience. Mayo Clin Proc 1990;65:1077-86. Back to cited text no. 39 |
| 40. | Beckwith JB. National Wilms Tumor Study: an update for pathologists. Pediatr Dev Pathol 1998;1:79-84. Back to cited text no. 40 [PUBMED] [FULLTEXT] |
| 41. | Brown HG, Kepner JL, Perlman EJ, Friedman HS, Strother DR, Duffner PK, et al. "Large cell/anaplastic" medulloblastomas:a Pediatric Oncology Group Study. J Neuropathol Exp Neurol 2000;59:857-65. Back to cited text no. 41 [PUBMED] [FULLTEXT] |
| 42. | Ellison D. Classifying the medulloblastoma: insights from morphology and molecular genetics. Neuropathol Appl Neurobiol 2002;28:257-82. Back to cited text no. 42 [PUBMED] [FULLTEXT] |
| 43. | Leonard JR, Cai DX, Rivet DJ, Kaufman BA, Park TS, Levy BK, et al. Large cell/anaplastic medulloblastomas and medullomyoblastomas: clinicopathological and genetic features. J Neurosurg 2001;95:82-8. Back to cited text no. 43 [PUBMED] |
| 44. | Eberhart CG, Cohen KJ, Tihan T, Goldthwaite PT, Burger PC. Medulloblastomas with systemic metastases: evaluation of tumor histopathology and clinical behavior in 23 patients. J Pediatr Hematol Oncol 2003;25:198-203. Back to cited text no. 44 [PUBMED] [FULLTEXT] |
| 45. | Eberhart CG, Kratz JE, Schuster A, Goldthwaite P, Cohen KJ, Perlman EJ, et al. Comparative genomic hybridization detects an increased number of chromosomal alterations in large cell/anaplastic medulloblastomas. Brain Pathol 2002;12:36-44. Back to cited text no. 45 [PUBMED] |
| 46. | Sarkar C, Roy S, Tandon PN. Primitive neuroectodermal tumours of the central nervous system--an electron microscopic and immunohistochemical study. Indian J Med Res 1989;90:91-102. Back to cited text no. 46 [PUBMED] |
| 47. | Caputy AJ, McCullough DC, Manz HJ, Patterson K, Hammock MK. A review of the factors influencing the prognosis of medulloblastoma. The importance of cell differentiation. J Neurosurg 1987;66:80-7. Back to cited text no. 47 [PUBMED] |
| 48. | Goldberg-Stern H, Gadoth N, Stern S, Cohen IJ, Zaizov R, Sandbank U. The prognostic significance of glial fibrillary acidic protein staining in medulloblastoma. Cancer 1991;68:568-73. Back to cited text no. 48 [PUBMED] |
| 49. | Janss AJ, Yachnis AT, Silber JH, Trojanowski JQ, Lee VM, Sutton LN, et al. Glial differentiation predicts poor clinical outcome in primitive neuroectodermal brain tumors. Ann Neurol 1996;39:481-9. Back to cited text no. 49 [PUBMED] |
| 50. | Packer RJ, Sutton LN, Rorke LB, Littman PA, Sposto R, Rosenstock JG, et al. Prognostic importance of cellular differentiation in medulloblastoma of childhood. J Neurosurg 1984;61:296-301. Back to cited text no. 50 [PUBMED] |
| 51. | Coffin CM, Braun JT, Wick MR, Dehner LP. A clinicopathologic and immunohistochemical analysis of 53 cases of medulloblastoma with emphasis on synaptophysin expression. Mod Pathol 1990;3:164-70. Back to cited text no. 51 [PUBMED] |
| 52. | Verma A, Sarkar C, Bhatia R, Banerji AK, Mehta VS, Mahapatra AK. Retrospective study of medulloblastoma with special reference to astrocytic differentiation - review of 63 cases. Neurol India 1993;41:7-12. Back to cited text no. 52 |
| 53. | Ito S, Hoshino T, Prados MD, Edwards MS. Cell kinetics of medulloblastomas. Cancer 1992;70:671-8. Back to cited text no. 53 [PUBMED] |
| 54. | Schiffer D, Cavalla P, Migheli A, Chio A, Giordana MT, Marino S, et al. Apoptosis and cell proliferation in human neuroepithelial tumors. Neurosci Lett 1995;195:81-4. Back to cited text no. 54 [PUBMED] [FULLTEXT] |
| 55. | Haslam RH, Lamborn KR, Becker LE, Israel MA. Tumor cell apoptosis present at diagnosis may predict treatment outcome for patients with medulloblastoma. J Pediatr Hematol Oncol 1998;20:520-7. Back to cited text no. 55 [PUBMED] [FULLTEXT] |
| 56. | Korshunov A, Golanov A, Ozerov S, Sycheva R. Prognostic value of tumor-associated antigens immunoreactivity and apoptosis in medulloblastomas. An analysis of 73 cases. Brain Tumor Pathol 1999;16:37-44. Back to cited text no. 56 [PUBMED] |
| 57. | Korshunov A, Savostikova M, Ozerov S. Immunohistochemical markers for prognosis of average-risk pediatric medulloblastomas. The effect of apoptotic index, TrkC and c-myc expression. J Neuro Oncol 2002;58:271-9. Back to cited text no. 57 |
| 58. | Eggert A, Grotzer MA, Zuzak TJ, Ikegaki N, Zhao H, Brodeur GM. Expression of Apo-3 and Apo-3L in primitive neuroectodermal tumours of the central and peripheral nervous system. Eur J Cancer 2002;38:92-8. Back to cited text no. 58 [PUBMED] [FULLTEXT] |
| 59. | Ramachandran C, Khatib Z, Escalon E, Fonseca HB, Jhabvala P, Medina LS, et al. Molecular studies in pediatric medulloblastomas. Brain Tumor Pathol 2002;19:15-22. Back to cited text no. 59 [PUBMED] |
| 60. | Brandes AA, Paris MK, Basso U. Medulloblastomas: do molecular and biologic markers indicate different prognoses and treatments? Expert Rev Anticancer Ther 2003;3:615-20. Back to cited text no. 60 [PUBMED] [FULLTEXT] |
| 61. | Ellison DW, Clifford SC, Gajjar A, Gilbertson RJ. What's new in neuro-oncology? Recent advances in medulloblastoma. Eur J Paediatr Neurol 2003;7:53-66. Back to cited text no. 61 [PUBMED] [FULLTEXT] |
| 62. | Gilbertson R, Wickramasinghe C, Hernan R, Balaji V, Hunt D, Jones-Wallace D, et al. Clinical and molecular stratification of disease risk in medulloblastoma. Br J Cancer 2001;85:705-12. Back to cited text no. 62 |
| 63. | Gilbertson R. Paediatric embryonic brain tumours biological and clinical relevance of molecular genetic abnormalities. Eur J Cancer 2002;38:675-85. Back to cited text no. 63 |
| 64. | Fisher PG, Burger PC, Eberhart CG. Biologic risk stratification of medulloblastoma: the real time is now. J Clin Oncol 2004;22:1-4. Back to cited text no. 64 |
| 65. | Packer RJ, Rood BR, Mac Donald TJ. Medulloblastoma: present concepts of stratification into risk groups. Pediatr Neurosurg 2003;39:60-7. Back to cited text no. 65 |
| 66. | Gilbertson RJ. Medulloblastoma: signalling a change in treatment. Lancet Oncol 2004;5:209-18. Back to cited text no. 66 |
| 67. | Cogen PH, Mc Donald JD. Tumour suppressor genes and medulloblastoma. J Neurooncol 1996;29:103-12. Back to cited text no. 67 |
| 68. | McDonald JD, Daneshvar L, Willert JR, Matsumura K, Waldman F, Cogen PH. Physical mapping of chromosome 17p13.3 in the region of a putative tumour suppressor gene important in medulloblastoma. Genomics 1994;23:229-32. Back to cited text no. 68 |
| 69. | Nicholson JC, Wickramasinghe CL, Ross FM, Crolla J, Ellison DW. Imbalances of chromosome 17 in medulloblastomas determined by comparative genomic hybridisation and fluorescence in situ hybridisation. Mol Path 2000;53:313-9. Back to cited text no. 69 |
| 70. | Scheurlen WG, Seranski P, Minchera A, Kuhl J, Sorensen N, Krauss J, et al. High resolution deletion mapping of chromosome arm 17p in childhood primitive neuroectodermal tumours reveals a common chromosomal disruption within the Smith-Magenis Region, an unstable region in chromosome band 17p11.2. Genes Chromosomes Cancer 1997;18:50-8. Back to cited text no. 70 |
| 71. | Steichen-Gersdorf E, Baumgartener M, Kerczy A, Maier H, Fink FM. Deletion mapping on chromosome 17p in medulloblastomas. Br J Cancer 1997;76:1284-7. Back to cited text no. 71 |
| 72. | Biegel JA, Janss AJ, Raffel C, Sutton L, Rorke LB, Harper JM, et al. Prognostic significance of chromosome 17p deletions in childhood primitive neuroectodermal tumors (medulloblastomas) of the central nervous system. Clin Cancer Res 1997;3:473-8. Back to cited text no. 72 |
| 73. | Bigner SH, Mark J, Friedman HS, Biegel JA, Bigner DD. Structural chromosomal abnormalities in human medulloblastoma. Cancer Genet Cytogenet 1988;30:91-101. Back to cited text no. 73 |
| 74. | Vagner C, Zattara C, Gambarelli D, Gentet JC, Genitori L, Lena G, et al. Detection of i(17q) chromosome by fluorescent in situ hybridisation (FISH) with interphase nuclei in medulloblastoma. Cancer Genet Cytogenet 1994;78:1-6. Back to cited text no. 74 |
| 75. | Batra SK, McLendon RE, Koo JS, Castelino-Prabhu S, Fuchs HE, Krischer JP, et al. Prognostic implications of chromosome 17p deletions in human medulloblastoma. J Neurooncol 1995;24:39-45. Back to cited text no. 75 |
| 76. | Scheurlen WG, Schwabe GC, Joos S, Mollenhauer J, Sorensen N, Kuhl J. Molecular analysis of childhood primitive neuroectodermal tumours defines markers associated with poor outcome. J Clin Oncol 1998;16:2478-85. Back to cited text no. 76 |
| 77. | Emadian SM, Mc Donald JD, Gerken SC, Fults D. Correlation of chromosome 17p loss with clinical outcome in medulloblastoma. Clin Cancer Res 1996;2:1559-64. Back to cited text no. 77 |
| 78. | Adesina AM, Nalbantoglu J, Cavenee WK. p53 gene mutation and mdm2 gene amplification are uncommon in medulloblastoma. Cancer Res 1994;54:5649-51. Back to cited text no. 78 |
| 79. | Saylors P, Sidransky D, Friedman H, Bigner S, Bigner D. Infrequent p53 gene mutations in medulloblastoma. Cancer Res 1991;51:4721-3. Back to cited text no. 79 |
| 80. | Woodburn RT, Azzarelli B, Montebello JF, Goss IE. Intense p53 staining is a valuable prognostic indicator for poor prognosis in medulloblastoma/central nervous system primitive neuroectodermal tumors. J Neurooncol 2001;52:57-62. Back to cited text no. 80 |
| 81. | Rood BR, Zhang H, Weitman DM, Cogen PH. Hypermethylation of HIC-1 and 17p allelic loss in medulloblastoma. Cancer Res 2002;62:3794-7. Back to cited text no. 81 |
| 82. | Aldosari N, Bigner SH, Burger PC, Becker L, Kepner JL, Friedman HS, et al. MYCC and MYCN oncogene amplification in medulloblastoma. A fluorescence in situ hybridization study on paraffin sections from the Children's Oncology Group. Arch Pathol Lab Med 2002;126:540-4. Back to cited text no. 82 |
| 83. | Avet-Loiseau H, Venuat AM, Terrier-Lacombe MJ, Lellouch-Tubiana A, Zerah M, Vassal G. Comparative genomic hybridization detects many recurrent imbalances in central nervous system primitive neuroectodermal tumours in children. Br J Cancer 1999;79:1843-7. Back to cited text no. 83 |
| 84. | Badiali M, Pession A, Basso G, Andreini L, Rigobello L, Galassi E, et al. N-myc and c-myc oncogenes amplification in medulloblastoma. Evidence of particularly aggressive behaviour of a tumour with c-myc amplification. Tumouri 1991;77:118-21. Back to cited text no. 84 |
| 85. | Bigner SH, Friedman HS, Vogelstein B, Oakes WJ, Bigner DD. Amplification of the c-myc gene in human medulloblastoma cell lines and xenografts. Cancer Res 1990;50:2347-50. Back to cited text no. 85 |
| 86. | Jay V, Squire J, Bayani J, Alkhani AM, Rutka JT, Zielenska M. Oncogene amplification in medulloblastoma: analysis of a case by comparative genomic hybridization and fluorescence in situ hybridization. Pathology 1999;31:337-44. Back to cited text no. 86 |
| 87. | Herms J, Neidt I, Luscher B, Sommer A, Schurmann P, Schroder T, et al. C-MYC expression in medulloblastoma and its prognostic value. Int J Cancer 2000;89:395-402. Back to cited text no. 87 |
| 88. | Grotzer MA, Hogarty MD, Janss AJ, Liu X, Zhao H, Eggert A, et al. MYC messenger RNA expression predicts survival outcome in childhood primitive neuroectodermal tumor/ medulloblastoma. Clin Cancer Res 2001;7:2425-33. Back to cited text no. 88 |
| 89. | Bruggers CS, Tai KF, Murdock T, Sivak L, Le K, Perkins SL, et al. Expression of the c-Myc protein in childhood medulloblastoma. J Pediatr Hematol Oncol 1998;20:18-25. Back to cited text no. 89 |
| 90. | Moriuchi S, Shimizu K, Miyao Y, Hayakawa T. An immunohistochemical analysis of medulloblastoma and PNET with emphasis on N-myc protein expression. Anticancer Res 1996;16:2687-92. Back to cited text no. 90 |
| 91. | Blaeker H, Rasheed BK, McLendon RE, Friedman HS, Batra SK, Fuchs HE, et al. Microsatellite analysis of childhood brain tumours. Genes Chromosome Cancer 1996;15:54-63. Back to cited text no. 91 |
| 92. | Kraus JA, Koch A, Albrecht S, von Deimling A, Wiestler OD, Pietsch T. Loss of heterozygosity at locus F 13B on chromosome 1 Q in human medulloblastoma. Int J Cancer 1996;67:11-5. Back to cited text no. 92 |
| 93. | Reardon DA, Michalkiewicz E, Boyett JM, Sublett JE, Entrekin RE, Ragsdale ST, et al. Extensive genomic abnormalities in childhood medulloblastoma by comparative genomic hybridisation. Cancer Res 1997;57:4042-7. Back to cited text no. 93 |
| 94. | Thomas GA, Raffel C. Loss of heterozygosity on 6q, 16q and 17p in human central nervous system primitive neuroectodermal tumors. Cancer 1991;51:639-43. Back to cited text no. 94 |
| 95. | Lusher ME, Lindsey JC, Latif F, Pearson AD, Ellison DW, Clifford SC. Biallelic epigenetic inactivation of the RASSF1A tumor suppressor gene in medulloblastoma development. Cancer Res 2002;62:5906-11. Back to cited text no. 95 |
| 96. | Tong CY, Hui AB, Yin XL, Pang JC, Zhu XL, Poon WS, et al. Detection of oncogenes amplifications in medulloblastomas by comparative genomic hybridization and array-based comparative genomic hybridization. J Neurosurg Spine 2004;100:187-93. Back to cited text no. 96 |
| 97. | Pomeroy SL, Tamayo P, Gaasenbeek M, Sturla LM, Angelo M, McLaughlin ME, et al. Prediction of central nervous system embryonal tumour outcome based on gene expression. Nature 2002;415:436-42. Back to cited text no. 97 |
| 98. | MacDonald TJ, Brown KM, LaFleur B, Peterson K, Lawlor C, Chen Y, et al. Expression profiling of medulloblastoma: PDGFRA and the RAS/MAPK pathway as therapeutic targets for metastatic disease. Nat Genet 2001;29:143-52. Back to cited text no. 98 |
| 99. | Barbacid M. Neurotropic factors and their receptors. Curr Opin Cell Biol 1995;7:148-55. Back to cited text no. 99 |
| 100. | Huang EJ, Reichardt LF. Neurotrophins: roles in neuronal development and function. Annu Rev Neurosci 2001;24:677-736. Back to cited text no. 100 |
| 101. | Minichiello L, Klein R. TrkB and TrkC neurotrophin receptors cooperate in promoting survival of hippocampal and cerebellar granule neurons. Genes Dev 1996;10:2849-58. Back to cited text no. 101 |
| 102. | Tajima Y, Molina RP Jr, Rorke LB, Kaplan DR, Radeke M, Feinstein SC, et al. Neurotrophins and neuronal versus glial differentiation in medulloblastomas and other pediatric brain tumors. Acta Neuropathol (Berl) 1998;95:325-32. Back to cited text no. 102 |
| 103. | Washiyama K, Muragaki Y, Rorke LB, Lee VM, Feinstein SC, Radeke MJ, et al. Neurotrophin and neurotrophin receptor proteins in medulloblastomas and other primitive neuroectodermal tumors of the pediatric central nervous system. Am J Pathol 1996;148:929-40. Back to cited text no. 103 |
| 104. | Segal RA, Goumnerova LC, Kwon YK, Stiles CD, Pomeroy SL. Expression of the neurotrophin receptor TrkC is linked to a favourable outcome in medulloblastoma. Proc Natl Acad Sci USA 1994;91:12867-71. Back to cited text no. 104 |
| 105. | Kim JY, Sutton ME, Lu DJ, Cho TA, Goumnerova LC, Goritchenko L, et al. Activation of neurotrophin-3 receptor TrkC induces apoptosis in medulloblastomas. Cancer Res 1999;59:711-9. Back to cited text no. 105 |
| 106. | Grotzer MA, Janss AJ, Fung K, Biegel JA, Sutton LN, Rorke LB, et al. TrkC expression predicts good clinical outcome in primitive neuroectodermal brain tumours. J Clin Oncol 2000;18:1027-35. Back to cited text no. 106 |
| 107. | Gilbertson RJ, Clifford SC, MacMeekin W, Meekin W, Wright C, Perry RH, et al. Expression of the ErbB-neuregulin signalling network during human cerebellar development: implications for the biology of medulloblastoma. Cancer Res 1998;58:3932-41. Back to cited text no. 107 |
| 108. | Rio C, Rieff HI, Qi P, Khurana TS, Corfas G. Neuregulin and ErbB receptors play a critical role in neuronal migration. Neuron 1997;19:39-50. Back to cited text no. 108 |
| 109. | Gilbertson RJ, Jaros EB, Perry RH, Pearson AD. Prognostic factors in medulloblastoma. Lancet 1992;340:480. Back to cited text no. 109 |
| 110. | Gilbertson RJ, Pearson AD, Perry RH, Jaros E, Kelly PJ. Prognostic significance of the c-ErbB-2 oncogene product in childhood medulloblastoma. Br J Cancer 1995;71:473-7. Back to cited text no. 110 |
| 111. | Gilbertson RJ, Perry RH, Kelly PJ, Pearson AD, Lunec J. Prognostic significance of HER2 and HER4 coexpression in childhood medulloblastoma. Cancer Res 1997;57:3272-80. Back to cited text no. 111 |
| 112. | Herms JW, Behnke J, Bergmann M, Christen HJ, Kolb R, Wilkening M, et al. Potential prognostic value of C-ErbB-2 expression in medulloblastomas in very young children. J Pediatr Hematol Oncol 1997;19:510-5. Back to cited text no. 112 |
| 113. | Wechsler-Reya RJ, Scott MP. Control of neuronal precursor proliferation in the cerebellum by Sonic Hedgehog. Neuron 1999;22:103-14. Back to cited text no. 113 |
| 114. | Hahn H, Wicking C, Zaphiropoulous PG, Gailani MR, Shanley S, Chidambaram A, et al. Mutations of the human homologue of Drosophila patched in the nevoid basal cell carcinoma syndrome. Cell 1996;85:841-51. Back to cited text no. 114 |
| 115. | Dean M. Polarity, proliferation and the hedgehog pathway. Nat Genet 1996;14:245-7. Back to cited text no. 115 |
| 116. | Reifenberger GJ, Wiestler OD, Chenevix-Trench G. NBCSS. In: Kleihues P, Cavenee WK (editors). World Health Organization Classification of Tumours, Pathology and Genetics of Tumours of the Nervous System. Lyon, France: IARC Press; 2000. p. 240-1. Back to cited text no. 116 |
| 117. | Raffel C, Jenkins RB, Frederick L, Hebrink D, Alderete B, Fults DW, et al. Sporadic medulloblastomas contain PTCH mutations. Cancer Res 1997;57:842-5. Back to cited text no. 117 |
| 118. | Vorechovsky I, Tingby O, Hartman M, Stromberg B, Nister M, Collins VP, et al. Somatic mutations in the human homologue of Drosophila patched in primitive neuroectodermal tumours. Oncogene 1997;15:361-6. Back to cited text no. 118 |
| 119. | Wolter M, Reifenberger J, Sommer C, Ruzicka T, Reifenberger G. Mutations in the human homologue of the Drosophilia segment polarity gene patched (PTCH) in sporadic basal cell carcinomas of the skin and primitive neuroectodermal tumours of the central nervous system. Cancer Res 1997;57:2581-5. Back to cited text no. 119 |
| 120. | Evans DG, Farndon PA, Burnell LD, Gattamaneni HR, Birch JM. The incidence of Gorlin syndrome in 173 consecutive cases of medulloblastoma. Br J Cancer 1991;64:959-61. Back to cited text no. 120 |
| 121. | Pietsch T, Waha A, Koch A, Kraus J, Albrecht S, Tonn J, et al. Medulloblastomas of the desmoplastic variant carry mutations of the human homologue of the Drosophilia patched. Cancer Res 1997;57:2085-8. Back to cited text no. 121 |
| 122. | Hart MJ, de los Santos R, Albert IN, Rubinfeld B, Polakis P. Downregulation of beta-catenin by human Axin and its association with the APC tumor suppressor, beta-catenin and GSK3 beta. Curr Biol 1998;8:573-81. Back to cited text no. 122 |
| 123. | Patapoutian A, Reichardt LF. Roles of Wnt proteins in neural development and maintenance. Curr Opin Neurobiol 2000;10:392-9. Back to cited text no. 123 |
| 124. | Eberhart CG, Tihan T, Burger PC. Nuclear localisation and mutation of beta-catenin in medulloblastomas. J Neuropathol Exp Neurol 2000;59:333-7. Back to cited text no. 124 |
| 125. | Huang H, Mahler-Araujo BM, Sankila A, Chimelli L, Yonekawa Y, Kleihues P, et al. APC mutations in sporadic medulloblastomas. Am J Pathol 2000;156:433-7. Back to cited text no. 125 |
| 126. | Mori T, Nagase H, Horii A, Miyoshi Y, Shimano T, Nakatsuru S, et al. Germ-line and somatic mutations of the APC gene in patients with Turcot syndrome and analysis of APC mutations in brain tumours. Genes Chromosomes Cancer 1994;9:168-72. Back to cited text no. 126 |
| 127. | Zurawel RH, Allen C, Chiappa S, Cato W, Biegel J, Cogen P, et al. Analysis of PTCH/SMO/SHH pathway genes in medulloblastoma. Genes Chromosome Cancer 2000;27:44-51. Back to cited text no. 127 |
| 128. | Zurawel RH, Chiappa SA, Allen C, Raffel C. Sporadic medulloblastomas contain oncogenic beta-catenin mutations. Cancer Res 1998;58:896-9. Back to cited text no. 128 |
| 129. | Cavenee WK, Burger PC, van Meir EG. Turcot syndrome. In : Kleihues P, Cavenee WK (editors). World Health Organization Classification of Tumours, Pathology and Genetics of Tumours of the Nervous System. Lyon, France: IARC Press; 2000. p. 238-9. Back to cited text no. 129 |
| 130. | Taipale J, Chen JK, Cooper MK, Wang B, Mann RK, Milenkovic L, et al. Effects of oncogenic mutations in Smoothened and Patched can be reversed by cyclopamine. Nature 2000;406:1005-9. Back to cited text no. 130 |
Copyright 2006 - Neurology India
The following images related to this document are available:
Photo images
[ni06003t1.jpg]
[ni06003t2.jpg]
|

{kind=link}
{kind=link}