 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
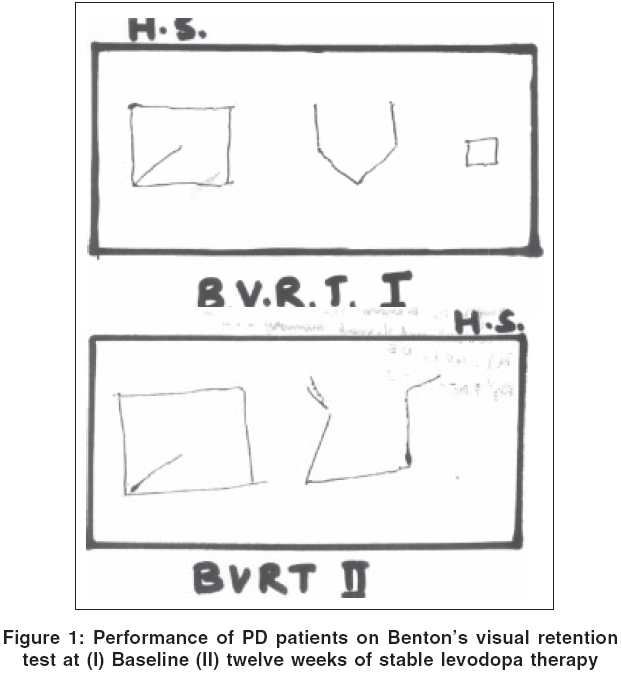
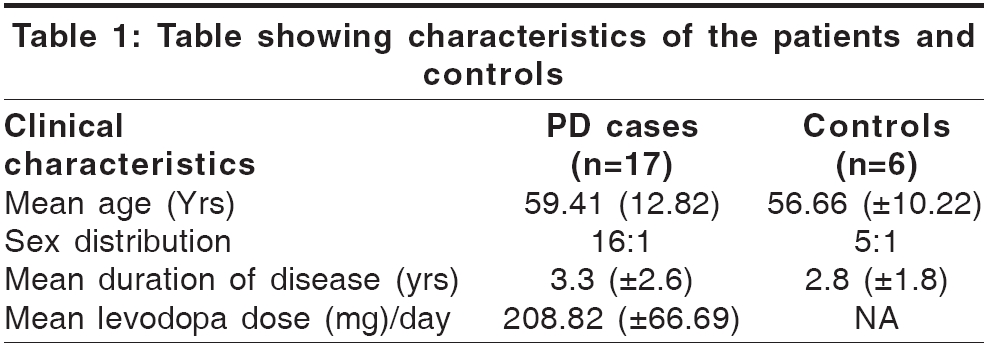
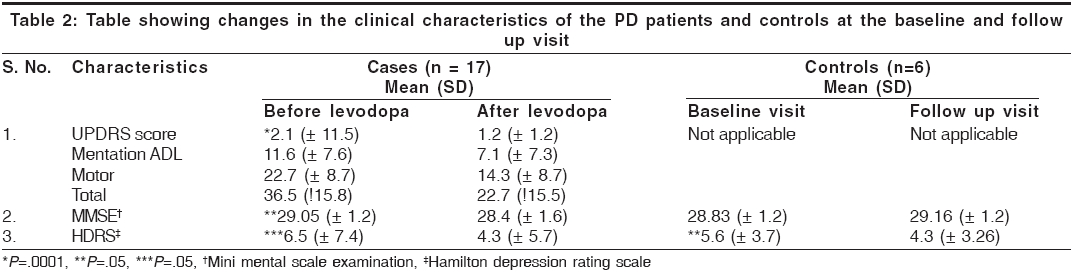
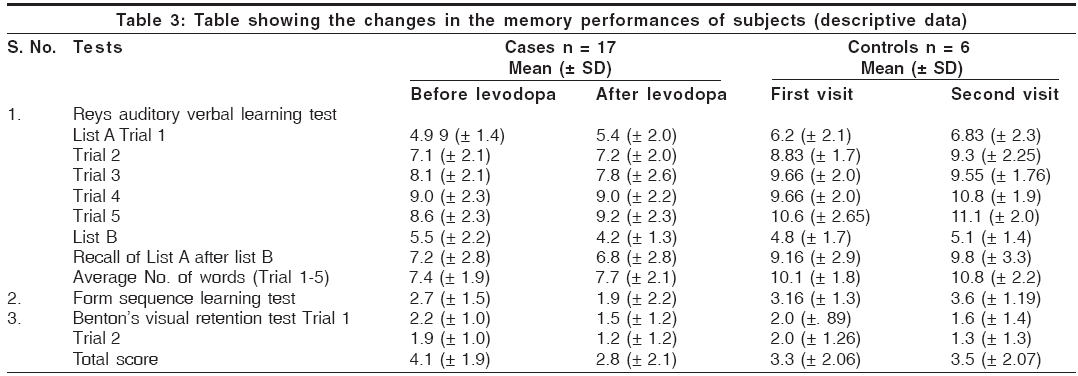
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 33-37 Original Article Verbal and visual memory in patients with early Parkinson's disease: Effect of levodopa Singh Sumit, Behari Madhuri Department of Neurology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110029 Code Number: ni06006 Abstract Background: The effect of initiation of levodopa therapy on the memory functions in patients with Parkinson's disease remains poorly understood.Aims: To evaluate the effect of initiation of levodopa therapy on memory, in patients with early Parkinson's disease. Settings and Design: Prospective case control study. Materials and Methods: Seventeen patients with early Parkinson's disease were evaluated for verbal memory using Rey's auditory verbal learning test, and visual memory using the Benton's visual retention test and Form sequence learning test. UPDRS scores, Hoehn and Yahr's Staging and Schwab and England scores of Activities of daily living. Hamilton's depression rating scale and MMSE were also evaluated. Six controls were also evaluated according to similar study protocol. Levodopa was then prescribed to the cases. Same tests were repeated on all the subjects after 12 weeks. Results: The mean age of the patients was 59.8 ( + 12.9 yrs); mean disease duration of 3.26 ( + 2.06 yrs). The mean UPDRS scores of patients were 36.52 ( + 15.84). Controls were of a similar age and sex distribution. A statistically significant improvement in the scores on the UPDRS, Hamilton's depression scale, Schwab and England scale, and a statistically significant deterioration in the scores of visual memory was observed in patients with PD after starting levodopa, as compared to their baseline scores. There was no correlation between degree of deterioration and the dose of levodopa. Conclusion: Initiation of levodopa therapy in patients with early and stable Parkinson's disease is associated with deterioration in visual memory functions, with relative preservation of the verbal memory. Keywords: Parkinson′s, levodopa, memory, Rey′s, benton, form Introduction Early Parkinson′s disease (PD) patients might show impairment in the neuropsychological tests[1],[2] despite overt dementia being reported only in 10- 30% PD patients.[1],[3],[4] The response of these impairments to treatment is not well established. Levodopa, undoubtedly, is the most effective drug in the management of the motor symptoms in PD but the effect of levodopa on memory functions remains controversial, with reports varying from improvement,[5] impairment,[6] and no change.[7] These controversies are probably due to difference in the methodology, patient selection, the tests used for such evaluations and the stage of the disease. Depression, reported in up-to 50% of PD patients,[2] can also interfere with the performance of patients on the neuropsychological tests and interfere with interpretation of the results. From the above account it becomes evident that the issue of memory functions in PD patients needs to be addressed in greater detail as this remains an open ended question. The present study was carried out with the objective of evaluating the effect of levodopa on memory in levodopa naive patients with early PD, with a hypothesis that initiation of levodopa therapy in these patients would either improve, or cause no change in the memory functions of patients [Figure - 1].Materials and Methods The study was an open label prospective study, conducted at All India Institute of Medical Sciences, New Delhi, India from June1997 to Dec 1999. The institutional ethics committee clearance was taken prior to the study. Inclusion criteria for the patients included patients with early PD, Hohen and Yahr′s stage 2.5 or less (United Kingdom Parkinson′s Disease Society, Brain bank diagnostic criteria)[8] when the treating physician considered it necessary to start them on levodopa. Informed consent was taken from the patients before including in the study. Exclusion criteria were patients with significant dementia, depression, past history of stroke, significant head injury or receiving levodopa or antipsychotic medications. Controls: Controls were individuals with other movement disorders, age and sex matched, attending the movement disorder clinic and not on levodopa. Study protocol Clinical evaluation The cases and the controls were assessed additionally using Memory tests Visual memory tests After the above tests, the PD patients were started on levodopa. The dose was maintained at a level as decided by the treating physician and the study protocol was re-administered after twelve weeks of the patients achieving a stable dose of levodopa. The controls were also subjected to the same protocol. Of the nineteen PD patients and six controls enrolled, seventeen PD patients and all the controls completed the study. Statistical analysis Results The mean age of the cases was 59.4 ± 12.82 years with a male: female ratio of 16:1. Seventy six percent (13) patients had symptoms for less than four years and the mean duration of the illness for the cases was 3.3 years (± 2.6 years). The mean age of the controls was 56.66 (± 9.03 years) and 83% of the controls were males [Table - 1]. Of the controls, 5 (75%) were receiving trihexiphenydyl and most of them were on more than one drug for the control of their movement disorders. Most of the cases were in stage I or stage II of the disease. None of the cases had significant dementia and one patient had mild depression. The changes in the clinical characteristics of the subjects between the baseline and follow up visits are shown in [Table - 2]. There was a statistically significant improvement in the mean UPDRS and HAMD rating scale scores in cases. A mild but statistically significant deterioration in the MMSE was also observed pertaining to the serial seven test in the MMSE. The controls showed a statistically significant improvement in their HAMD rating scale scores but not in their MMSE scores. The mean values of the raw data of the cases and the controls exhibiting their performance on the memory functions were analysed. The verbal memory scores did not show any significant change before and after levodopa. Indeed, the average numbers of recalls were slightly more in the "after" evaluation [Table - 3]. There was a statistically significant deterioration in the visual memory scores in PD patients after starting levodopa, which was not reflected in the verbal memory scores [Table - 4]. In contrast to these findings, the controls demonstrated no change in their visual memory scores but there was a statistically significant improvement in their verbal memory scores. There was no correlation between the memory functions and the dose of levodopa. Discussion This study shows that the initiation of levodopa therapy in patients with early and stable PD is associated with deterioration in their performance on tests of visual memory. This finding was rather unexpected and against our hypothesis formulated at the beginning of the study. The test for visual memory, used in this study required the motor capabilities of patients to draw. A statistically significant improvement in the UPDRS scores of the patients′ makes impairment in motor function unlikely to be the cause of this deterioration in memory tests. In the present study the PD patients acted as their own controls in the ′test-intervention-retest′ design of the study. In order to strengthen our findings, the controls were taken and were also evaluated according to the same protocol to obviate the bias produced by ′learning effect′. Drugs, co administered with levodopa were unlikely to be responsible for deterioration in the memory functions. Anticholinergic drugs have been reported to cause an acute confusional state in patients with long standing PD.[12] Our patients, with early PD, were on a stable dose of anticholinergic medication which stayed unchanged till the end of the study. Selegiline, the other drug taken by the patients, has not been reported to be associated with deterioration in memory in PD.[13] Thus we attribute this impaired visual memory in patients to levodopa indeed as this was the only new drug introduced. Most studies evaluate the performance of PD patients on tasks of memory by evaluation of the reaction time. We chose to eliminate the time factor completely by scoring their performance on the accuracy of their response, instead of the time taken, which could be a confounding factor after improvement in the motor performance of the patients once levodopa was started. Previous studies have found impairment, in verbal and visual memory[14] in PD patients as the disease progresses. These studies included patients with a longer duration of the disease (6.62 yrs as compared to 3.2 yrs in our study). These studies probably indicate the natural course of the disease where patients with PD can develop abnormalities of memory functions with time. In the present study the re-evaluation was done only after 12 weeks, which is too short a duration to cause a significant deterioration in the severity of the disease. Kulisewsky et al[15] found deterioration in verbal and visual memory in the subset of PD patients with a "wearing off" phenomenon to levodopa. The authors have studied both visual and verbal memory by presenting visual material. We, on the other hand have studied visual memory by providing tests containing retention of visual material, and verbal memory by giving verbal tests. It is therefore possible that the deterioration in verbal memory observed by those authors could be a reflection of altered visual memory itself. The impairment of visual memory has been reported in other studies too, which have studied high speed memory scanning[6] and memory to visually presented material. Kulisewsky et al[16] have reported an improvement in the performance of the patients with early PD on memory tasks, which begin at 6 months. It is possible that the deterioration observed after starting levodopa in early PD might improve with time. Working memory tasks have been reported to be more sensitive to dopaminergic activity than the performance on the storage and recall memory tests. Copper et al[17] have reported short term memory deficits in PD patients, and these deficits do not respond to treatment. Therefore we chose to test the performance of our patients on tasks of recall based memory (episodic memory) instead of working memory. D1 dopamine receptors and there connections with the prefrontal cortex are said to be intimately involved in the memory functions.[18] There are two different internuclear connections within the basal ganglia. The direct pathway is excitatory and indirect pathway is inhibitory to the cortex. The indirect pathway, proposed to be associated with the visual memory might be relatively dopamine preserved in the early phase and exogenous dopamine administered to these patients might cause an over stimulation of these connections, thereby causing deterioration in the performance of patients on the visual memory functions, while sparing the verbal memory. Frank[19] has proposed a similar model for impaired cognitive functions in PD patients on levodopa. It is also possible that impaired executive functions in PD patients, after starting levodopa might contribute such impairments in visual memory.[20] A small sample size and an unconventional method of evaluation of the neuropsychological tests are the shortcomings of our study, as is the lower number of the controls. Our study points towards a dopaminergic substrate for memory deficits in PD patients. It also highlights that the deterioration in the memory, which we found in our patients, could be due to exposure of the partially preserved dopaminergic system in early PD, to relatively higher doses of levodopa. This underscores the importance of starting the treatment in early PD with a relatively lower dose of levodopa. Larger randomised controlled trials may be of benefit in resolving the issue of memory functions in PD patients in future and there importance cannot be overemphasised. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06006t4.jpg] [ni06006t2.jpg] [ni06006t1.jpg] [ni06006t3.jpg] [ni06006f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}