 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
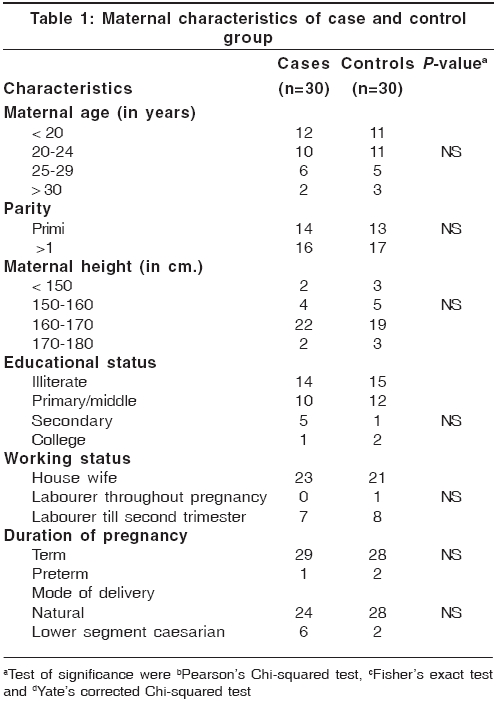
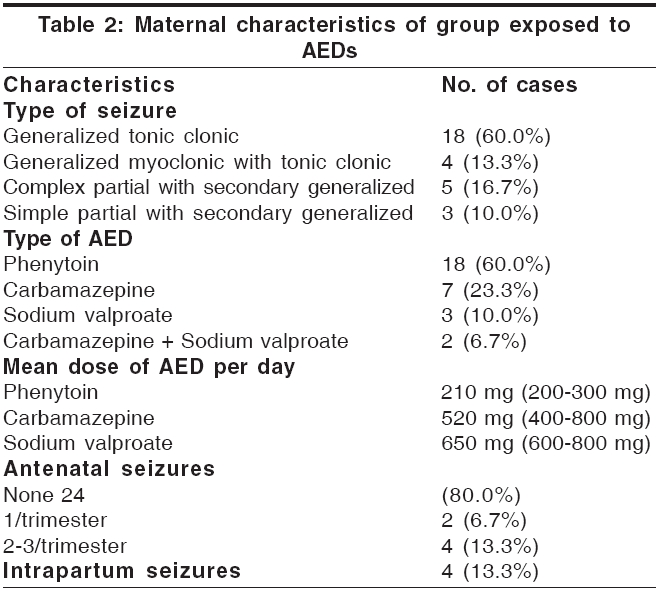
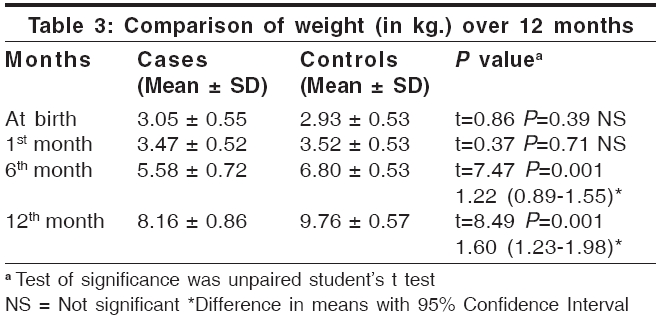
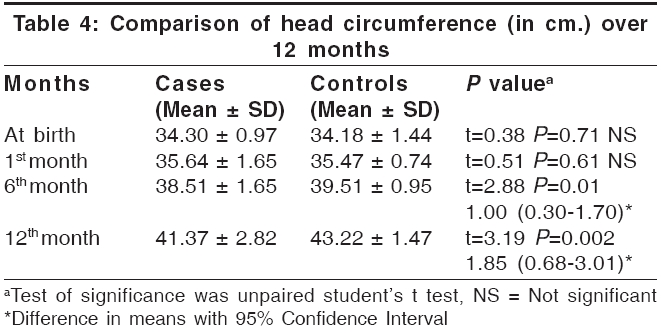
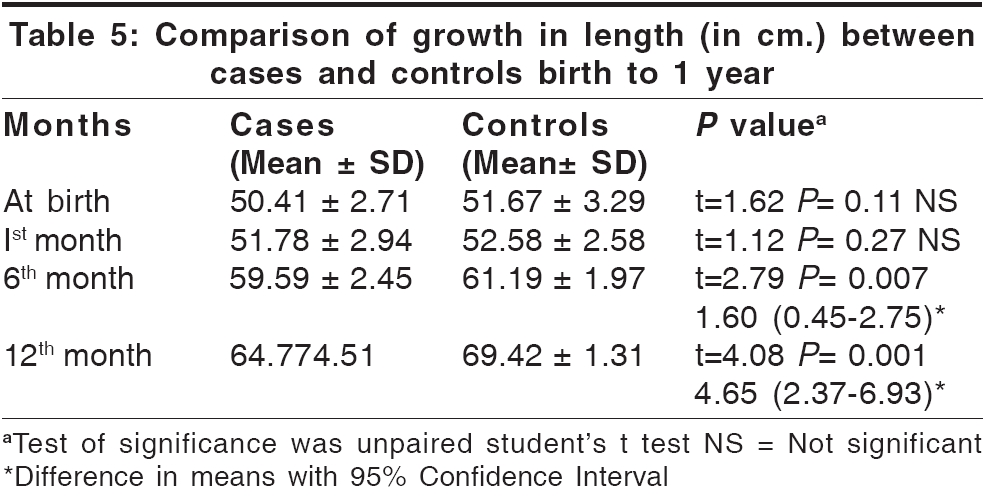
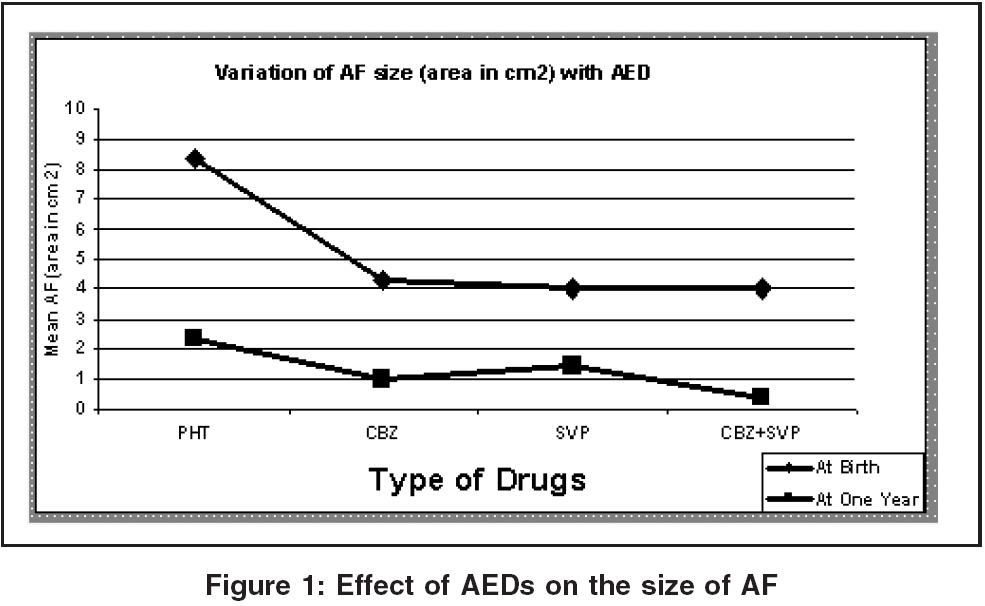
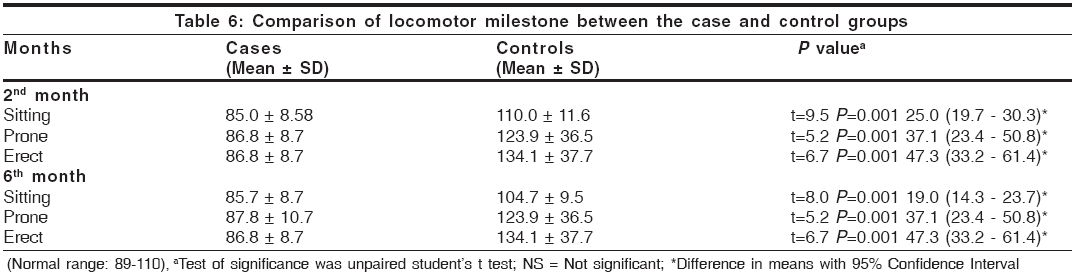
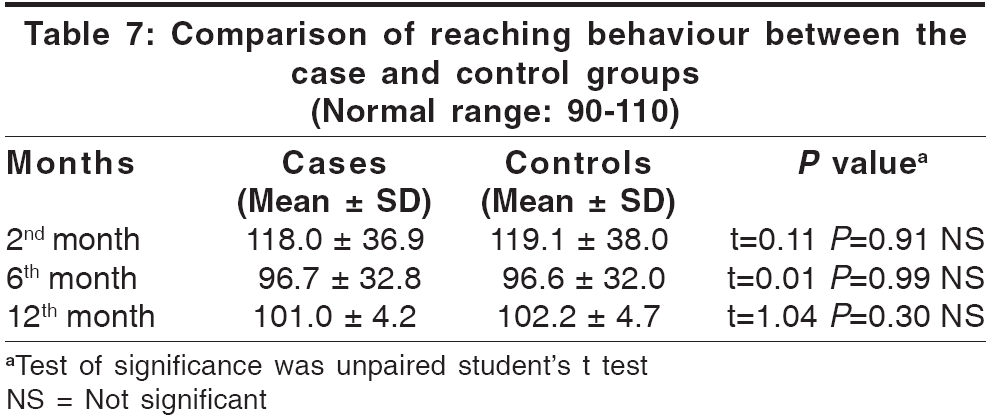
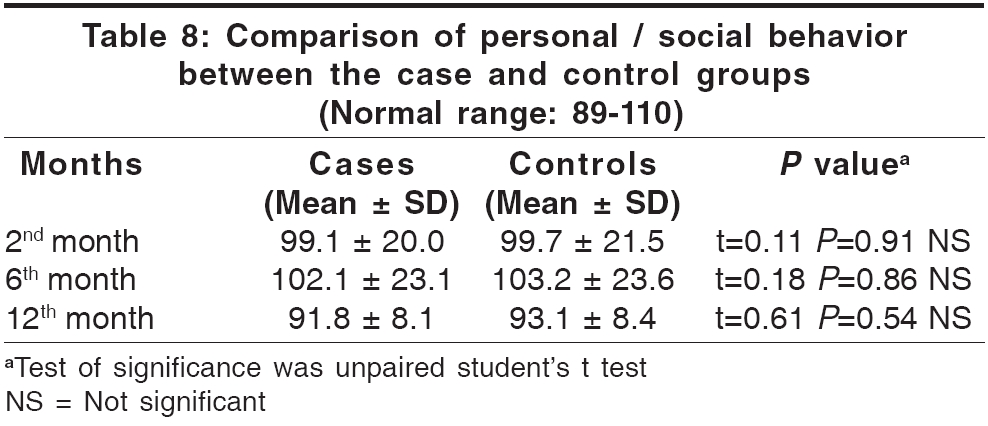
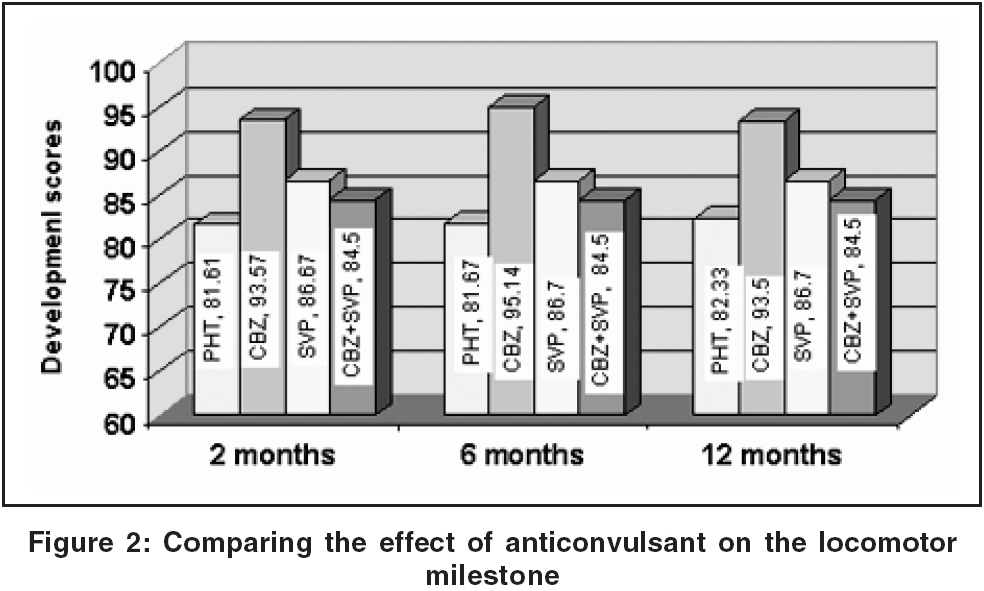
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 42-46 Original Article Physical growth and psychomotor development of infants exposed to antiepileptic drugs in utero Arulmozhi T, Dhanaraj M, Rangaraj R, Vengatesan A Departments of Neurology, Government Stanley Medical College and Hospital, Chennai Code Number: ni06008 Related article: ni06009 Abstract Objective: To evaluates the physical growth and psychomotor development of infants born to women with epilepsy on regular Anti Epileptic Drugs (AEDs).Setting: Govt. Stanley Medical College and Hospital, Tertiary care referral centre, Chennai. Design: Open prospective cohort study with a control group. Materials and Methods: Consecutive women with epilepsy who were on regular anticonvulsants were followed up from their first trimester. Their babies were examined at birth and anthropometric measurements including anterior fontanelle size were noted. They were followed up till one year and periodically evaluated at 1st, 6th and 12th month of age. Development testing using Griffith scale was done at 2nd, 6th and 12th month. An equal number of control babies were also studied using the same scale for one year at the specified intervals. The results in both the groups were compared. Results : 30 babies were enrolled in the case and control group. The AEDs received by the mothers with epilepsy were Phenytoin, Carbamazepine, and Sodium valproate. At birth and 1st month the weight, head circumference and length of case and control babies were equal. At 6th and 12th month reduction in the above 3 parameters were noted in the case babies ( P <0.01). Area of anterior fontanelle (AF) was larger in the study group particularly in those exposed to phenytoin in utero( P <0.001). In the case babies reduction in the sitting, prone and erect progression of the locomotor scores was observed at 2nd month ( P <0.001). Prone progression alone improved by 12th month and other two remained less than the control ( P <0.001). No difference was observed in reaching behaviour and personal/social scores in both groups. Infants exposed to Phenytoin monotherapy had a negative impact on sitting progression. Conclusion : Among infants exposed to AEDs in utero physical growth was equal to that of control at birth but reduced at 6th and 12th month probably due to extraneous factors. The Locomotor scores showed reduction in all areas in 2nd, 6th and 12th month except prone progression which alone improved by 12th month. Phenytoin exposure in utero resulted in large AF and it had a negative impact on sitting progression in comparison with Carbamazepine and Sodium valproate. Keywords: Antiepileptic drugs (AEDs), anterior fontanelle Introduction The impact of antiepileptic drugs (AEDs) taken by women with epilepsy during pregnancy on the children born to them remains an issue of debate, despite decades of concern and research.[1] The immediate harmful effects of AEDs in pregnancy manifesting as congenital anomalies are well known.[2],[3] Recently more studies are focusing on the long-term effects on growth and developments among children exposed AEDs in utero.[4],[5],[6],[7],[8] There are hardly any long term follow up studies of the babies born to mothers with epilepsy in the Indian literature. This information would be of vital use in choosing the appropriate anti-epileptic drug during pregnancy, early identification of developmental delays and growth abnormalities and offering timely intervention. It would also help in achieving the highest developmental potential of these at risk babies. In this paper the growth and development pattern of the infants exposed to antiepileptic drugs in utero are highlighted.Materials and Methods This is an open prospective study, done for a period of 2 years from January 2002. All consecutive women with epilepsy in the reproductive age, already on anticonvulsant drugs and attending regularly the Neurology Out patient clinic were recruited when they became pregnant. Those who reported their pregnancy after the first trimester were excluded from the study. The mothers were initially evaluated by a neurologist and appropriate anticonvulsant based on the seizure type was started prior to conception. The drugs used were phenytoin, carbamazepine and sodium valproate. Monotherapy was preferred as a rule. The dosage of the anti convulsants were adjusted if needed. Folic acid 5 mg per day was advised prior to conception itself. All the mothers were referred to the nearby Government RSRM hospital, which is a part of Government Stanley hospital for antenatal checkup and confinement. Fetal ultra sonogram was done by 20 weeks of pregnancy. They were followed till delivery and the data regarding - the duration of pregnancy, relapse of seizure, mode of delivery, APGAR scores, and anthropometric data at birth were collected and noted in a data sheet. The babies were examined at 1st, 2nd, 6th and at 12th month of age. Physical growth was assessed by measuring the body weight, head circumference, length, and anterior fontanelle. The body weight was recorded to the nearest of 0.1 kg on a standardized beam balance without clothes; Birth weight was measured within the first hour before significant post natal weight loss had occurred; Length was measured by an infantometer and head circumference with a flexible inch tape passing over the occipital protuberance, above the ears and supra orbital ridges and the area of the anterior fontanelle was recorded by multiplying the distances from the midpoint of the opposite sides.[9] The psychomotor development of the babies was assessed using the Griffiths′scale.[10] The babies were evaluated under the domains of locomotor, reaching behavior and personal -social development. The locomotor development was evaluated under the subsets of developmental sequences i.e., the sitting, prone and erect progression. For control, the babies born at Government RSRM hospital where most of the case babies were also born was selected. The first 2 babies born on every Saturday was selected till the adequate number was reached. The details were entered in the same proforma and followed up similarly. The controls were matched for socio economic status, education of the parents, nutritional status of the mothers and education. The mothers were interviewed regarding the feeding pattern of the child - whether breastfed or started on supplementary feeds and intercurrent illness if any was noted. Statistical analysis Results During the study period thirty three pregnant women with epilepsy were enrolled. One had abortion and two were lost in the follow up after delivery. (Among the 3 patients 2 had GTCS and one had complex partial with secondary generalized seizure; the first two were on phenytoin 200-250 mg daily and the third on carbamazepine 600mg per day). Hence this study consisted of 30 babies each in the study and control group and followed up for 12 months. The maternal characteristics such as age, parity and education are comparable and given in [Table - 1]. None of the mother belonging to both the groups had the habit of smoking, alcohol drinking or substance abuse. The details of the Seizure type and AEDs are given in [Table - 2]. Anti convulsants were started prior to conception itself. Seizures were fully controlled with no recurrence throughout pregnancy in 22(73%). The remaining 8(27%) had recurrence which was managed by increasing the dose of anticonvulsant. Intra partum seizures without any cause occurred in 4(13%). Emergency caesarian was done in 6(20%) of the study group and 2(6.7%) of the control group. The indications in the study group were fetal distress in 2 and intrapartum seizures in 4 whereas in the control group it was due to previous caesarian in both of them. The male female ratio of the babies was 14: 16 in the case and 13: 17 in the control group respectively. All babies in both groups had normal APGAR scores except one in the case group which was later diagnosed to have transposition of great vessels. Another baby had a minor anomaly in the form of polydactyly. Apart from this no major congenital anomalies were encountered in both the groups. The weight, head circumference and length of the case and control babies over 12 months are given in [Table - 3][Table - 4][Table - 5]. The mean weight of the case and control babies at birth and 1st month were equal. By 6th and 12th month the case babies had significant lower weight than the controls ( P < 0.001) [Table - 3]. At birth and 1st month the mean head circumferences of the case and control babies were almost equal (34.3 ± 0.97 cm and 34.18 ± 1.44cm respectively). But by 6th and 12th month the case babies had significant lower head circumference than the controls ( P < 0.01) [Table - 4]. The mean lengths of the case and control babies were 50.41 ± 2.71 cm and 51.67 ± 3.29 cm at birth which was equal in both groups. By 6th and 12th month the case babies had significant lower length than the controls ( P < 0.01) [Table - 5]. Critical analysis of Weight, Height and Head Circumference was done using 50th of percentile of control babies. Analysis of growth revealed that at one year 50% of the control babies were above 9.72 kg (50th percentile) whereas only 10% of the case babies were above this weight; for head circumference 43.6 cm (50th percentile) for control babies and 20% in case babies; for length 69.5 cm (50th percentile) and 20% in case babies. Thus all the three parameters were reduced in most of the case babies at the age of one year. The mean area of the anterior fontanelle at birth for case and control babies was 6.68 ± 3.97 cm and 1.92 ± 0.74 cm (t=6.46 P < 0.01) and at one year it was 1.78 ± 1.76 cm and 0.52 ± 0.76 cm (t= 3.59 P < 0.01). Thus in the case group it was significantly large at birth and at 1 year. On studying the effect of individual anticonvulsant it was significantly larger in those exposed to phenytoin in utero ( P < 0.001) [Figure - 1]. Metopic sutures was found in 7(23.3%) and suture widening in 4 (13.3%) of the case babies whereas it was not observed in control group. Posterior fontanelle was found to be patent in 3 (10%) compared to 1 (3.3%) in the control group at birth. Comparison of the developmental scores revealed a significant reduction in the locomotor milestones in all the 3 subtests of sitting, prone, and erect progression. at 2 months and at 6 months in the case babies ( P < 0.001). By 12th months the scores for the prone progression alone improved and no significant difference was observed [Table - 6]. The reaching behavior and personal/social scores were equal in both groups [Table - 7][Table - 8]. On studying the effect of antiepileptic drugs on the locomotor scores significant reduction was found in the sitting progression with phenytoin ( P < 0.001) [Figure - 2]. Discussion In this study except one all mothers had term delivery and is in agreement with the findings of the Kerala pregnancy registry.[11] In a study from Denmark a significant increase in preterm deliveries were observed and this has been attributed to maternal smoking habits rather than to AEDs per se.[12] The authors postulated that the interaction between antiestrogen activity of the nicotine and AEDs might be a factor for increased number of premature labour in their study. None of the mothers in our study were smokers. In our study the increased Caesarian rate was probably due to seizures in the first stage of labour and the incipient fetal distress. Major congenital anomaly was observed in only one baby. This is in contrast to the previous Indian study in which it was12%.[11] In the present study none of the babies exposed to AEDs in utero had significant reduction in birth weight. This was similar to the observations in some of the earlier studies.[2],[4] In the study from Kerala, 21.4% of the babies had low birth weight.[11] The Boston study by Holmes et al had also observed growth retardation in 10.8% of infants exposed to AEDs when compared to 4.1% in the control group.[3] In the Danish study the babies born to mothers who stopped AEDs during pregnancy and the babies born to mothers who continued to take AEDs during pregnancy had comparable birth weight. This the authors attributed to the severity of the disease and not to AEDs.[12] Follow-up weight gain of the babies at 6th and 12th month showed significant reduction in the case group. The growth in the head circumference also showed similar patter. This indicates that the babies in the case group probably faced some continuous extraneous factors during infancy, which impaired their weight gain. It could be inadequate breast feeding and or early weaning based on an unfounded fear of transmitting the disease or the adverse effect of AEDs to the babies, poor socioeconomic status, dietary restrictions on the lactating mother or frequent intercurrent illnesses of the babies. However we have not studied these factors in detail and this needs prospective studies, as they are unique to the Indian context and are largely amenable to social and educational intervention. Growth in length followed a different pattern when compared to weight and head circumference. There was a slight reduction in length in the babies in case group at birth, which attained significance at 6th and 12th month. Wide et al, found a significant reduction in weight, head circumference and length, which tended to improve towards the first year and was marked in babies exposed to polytherapy and also in babies exposed to carbamazepine monotherapy.[13] The present study suggests that the postnatal conditions may play a major role to play on the ultimate body dimensions at one year. The wide opened anterior fontanelle and metopic sutures observed at birth and tending to diminish at one year might be due to the effect of phenytoin on bone metabolism.[14] In our study this finding was significantly observed in infants born to mothers exposed to phenytoin than other AEDs. By one year this significance disappeared. These observations support the effect of phenytoin on metabolism. Prospective studies of calcium and vitamin D supplements in WWE are needed to clarify these issues. In the developmental domain a significant reduction in all the three aspects of locomotor scores were observed in the case babies at 2nd and 6th month. By 12th month the reductions persisted only in the sitting and erect progression but improved in prone progression. Among the AEDs, phenytoin alone had negative influence on sitting progression. In a population based longitudinal follow up study, Wide et al. using Griffiths scale did not observe any differences between the infants exposed to AEDs in utero and controls.[15] However the same authors noticed subtle but significant reduction in the locomotor development among children aged 41/2 - 5 years who were exposed to phenytoin in utero.[5] These children also had fewer siblings and their mothers had lower level of education. Hirano et al found that the development of infants was influenced by the effects of AEDs exposure in utero and occurrence of maternal seizure but in the subsequent years, child care environment such as maternal ability of child-rearing was the major influencing factor.[7] Assessment of specific cognitive functions and intelligence of children aged 5 years born to mothers with epilepsy also showed that the major influencing factors were maternal partial seizure, fetal asphyxia following generalized convulsions in the carrying mothers and low paternal education but not AED exposure in utero.[16] A genetic connection between epilepsy in the mother and poor intellectual performance in the child had also been observed.[17] Thus even though delay in locomotor score among infants exposed to AEDs in utero had been observed in few studies as in this series, the subsequent development by 5 years depended on the environmental factors, child-rearing methods and parental education rather than AED toxicity.[5],[7],[16],[17] To conclude this study has revealed an early restriction in the locomotor milestones and a delayed affection of physical growth parameters among the babies exposed to AEDs in utero. Various intrauterine and postnatal factors probably affected the development and growth parameters of these babies. It suggests an early intervention programme involving effective seizure control among the mothers with epilepsy during pregnancy, maternal nutrition, family education about epilepsy, AEDs, breast feeding and with regular monitoring of physical growth and cognitive skills of the babies. The limitation of the study is the small sample size particularly in the AED subgroups and non adjustment of the nutritional status of mothers between both groups. However all the mothers in the study and control group were uniformly from lower socio economic section. Hence future long term studies with larger sample size and consideration of the maternal nutritional status are required for better understanding of the problem. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06008t3.jpg] [ni06008t7.jpg] [ni06008t2.jpg] [ni06008t8.jpg] [ni06008t6.jpg] [ni06008t5.jpg] [ni06008f2.jpg] [ni06008t1.jpg] [ni06008f1.jpg] [ni06008t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}