 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
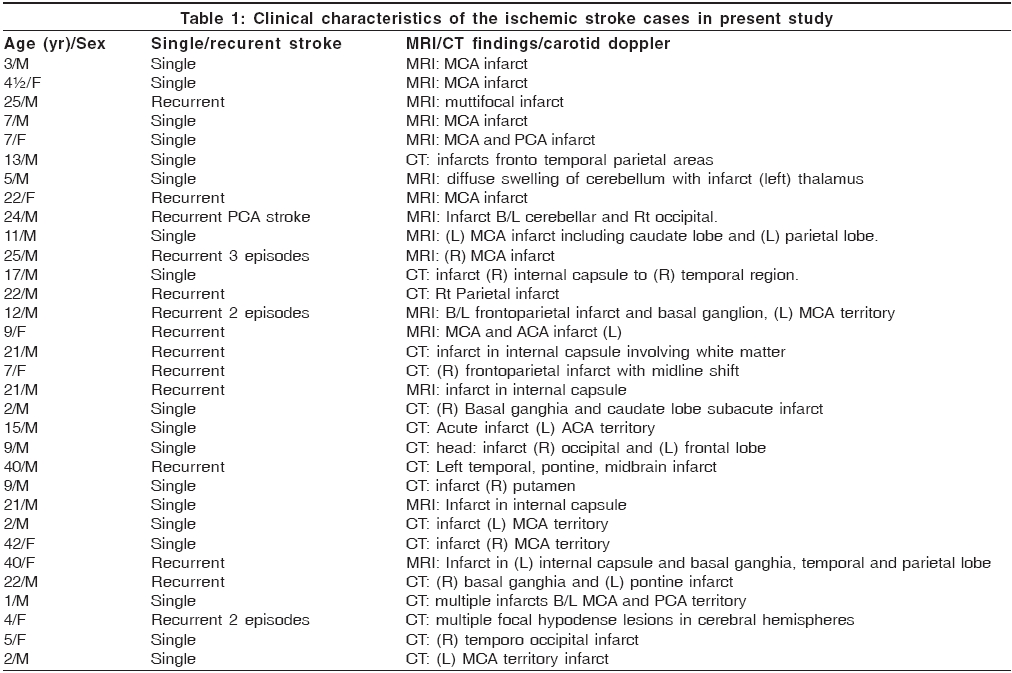
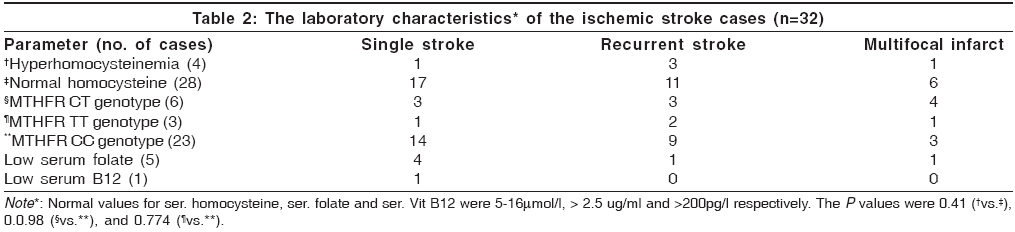
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 48-50 Original Article Role of MTHFR C677T polymorphism in ischemic stroke Panigrahi Inusha, Chatterjee Tathagata, Biswas Arijit, Behari Madhuri, Choudhry PrakashVed, Saxena Renu Departments of Hematology, All India Institute of Medical Sciences, Ansari Nagar, Delhi - 110 029 Code Number: ni06010 Related articles: ni06011, ni06012 Abstract Background: Homozygosity for MTHFR C677T polymorphism can lead to significantly high homocysteine levels and hyperhomocysteinemia is an important risk factor for thrombotic events.Aims: The aim was to determine role of MTHFR C677T polymorphism in North Indians with ischemic stroke. Settings and Design: In a prospective study, the subjects of stroke were recruited from the neurology clinic of the hospital. Controls were healthy individuals from the Hematology clinic without any history of stroke. Materials and Methods: Plasma homocysteine levels were measured by enzyme immuno assay method after 3 months of acute episode. Serum folate and Vitamin B12 levels were estimated by competitive inhibition radioassay. MTHFR polymorphism was detected by PCR-RFLP using Hinf I enzyme. Statistical analysis: The analysis of significance of results was done using SPSS software package. A pvalue < 0.05 was taken as significant. Results: Thirty-two acute ischemic stroke patients (aged 1-44 years) were studied. Fourteen (43.8%) had recurrent stroke. Nine (28%) had multiple infarcts. Four of 32 patients (12.5%) had high homocysteine levels. Three out of these 4 hyper-homocysteinemia patients were homozygous ( TT ) for MTHFR polymorphism (2 with recurrent stroke). Two of three homozygous cases with TT genotype had low serum folate. Five of 32 stroke cases (18.8%) were heterozygous ( CT ) genotype. Conclusions: Primary hyper-homocysteinemia appears to be an important risk factor for ischemic stroke in North Indians, most due to MTHFR C677T homozygosity. Folate levels may modify the presentation of the MTHFR TT genotype. Keywords: Asian-Indians, cerebrovascular disease, homocysteine, methylene tetrahydrofolate reductase. Introduction MTHFR C677T polymorphism results in reduced folate-dependent enzyme activity and reduced re-methylation of homocysteine to methionine. Homozygotes for this polymorphism have significantly higher homocysteine, an important predisposing factor for thrombosis. Present study was conducted to determine prevalence of hyper-homocysteinemia in North Indians with ischemic stroke and, to determine its relationship with MTHFR genotype, if any.Materials and Methods Subjects included consecutive cases of ischemic stroke attending the Neurology clinic of the hospital from June 2003 to May 2004, enrolled in the prospective study. Patients with ischemic stroke and no "traditional" risk factors were included. Inclusion criteria were, a) age < 45 years at presentation, and b) absence of history of smoking or significant systemic disease and intake of anti-epileptics, anti-cancer drugs or exogenous vitamins. Ischemic stroke was documented on MRI and/or CT. Recurrent stroke was defined as more than one episode of stroke at presentation, including the present episode at least 1 year apart. Sixty unrelated age and sex-matched healthy individuals from the Hematology clinic with no history of stroke, served as controls. Informed consent was taken from the patients or parents (in children < 10 years). The Institute ethical committee approved the study. Plasma homocysteine (Hcy) levels were measured on samples obtained 3 months after acute episode, by modified EIA (enzyme immuno assay) (Diazyme laboratories, San Diego, CA). Normal level of homocysteine was taken as 5-12 ìmol/l. Serum folate and Vitamin B12 levels were assayed by competitive inhibition radioassay (SimulTRAC, Becton Dickinson, Orangeberg, NY). The normal levels for folate and Vitamin B12 were taken as greater than 2.5 μmg/ml and 200ng/l respectively. The MTHFR C677T polymorphism was studied by PCR-RFLP on DNA samples,[1] using enzyme Hinf I . Statistical analysis was done by Fisher′s exact test and Chi Square test by SPSS software and p0 < 0.05 was taken as significant. Results Of thirty-two patients with ischemic stroke (M: F= 22:10; age 1-42 years, median 12 years) were studied [Table - 1]. Ten (31.3%) showed infarcts in MCA territory alone, and nine (28%) patients had multiple brain infarcts. Fourteen patients (43.8%) had recurrent stroke. High plasma homocysteine (>12 µmol/l) was seen in four of thirty-two (12.5%) [Table - 2], not seen in controls. Occurrence of hyper-homocysteinemia in patients was significant ( p0 = 0.02). MTHFR homozygous ( TT genotype) was seen in three patients but in none of controls ( P =0. 073). Youngest case was 25 years age and one had multiple brain infarcts. MTHFR CT (heterozygous) genotype was seen in six of 32 cases (18.8%) but 4/60 (6.6%) controls ( P = 0.16). None of heterozygous individuals showed high homocysteine. However, no significant association was found between single vs. recurrent stroke in patients with hyperhomocysteinemia ( P =0.41), MTHFR CT genotype ( P =0.98) and MTHFR TT genotype ( P =0.77). When single stroke, multiple stroke and multifocal infarct were considered with variables as high homocysteine, MTHFR TT genotype and CT genotype, the p value did not achieve significance. The number of cases in each group being less, the comparision between the groups did not show any significant difference. Discussion Studies in Caucasians have not shown correlation between MTHFR C677T polymorphism[2] and vascular disease. In present study, high incidence of heterozygosity (6.6%) was observed in controls. The ischemic stroke cases were young or middle aged patients, with median age of 12 years. Serum homocysteine concentration was significantly higher in TT genotype compared to CC (normal) and CT (heterozygous) genotypes,[3] in a Turkish study. The prevalence of homozygous gene mutation for MTHFR was high,[4] in Turkish stroke patients. In present study, 4/32 (12.5%) of young stroke had hyper-homocysteinemia, of which 3 had TT genotype. A previous Indian study has reported CT genotype,[5] in 54.5% patients with hyper-homocysteinemia and coronary artery disease (CAD). In study from Hyderabad,[6] TT genotype was found in only 1.4% of hyperhomocysteinemia cases with low background prevalence for heterozygosity (2.08%). In a study in Tamilians,[7] CT genotype (heterozygosity) was seen in 18.1%(13/72) and TT genotype in 1.38%. The MTHFR A1298C polymorphism is even more prevalent in Tamilians (47.2%). Some selection bias could have been due to analysis of a heterogenous population, comprising of 52 acute myocardial infarction cases and 20 normal individuals. In a study from Mumbai,[8] heterozygote frequency was high in CAD (38%) though comparable to controls (31%) and significant association with disease was found in females. In another study from Mumbai in venous thrombombolism,[9] CT and TT genotypes were present in 14.9% and 1.2%. Thus there is marked geographic variation in frequency of C677T polymorphism in Indians. Present study reflects high prevalence of MTHFR polymorphism in North Indians and a relatively greater contribution to hyperhomocysteinemia especially in young aged 20-40 years. All three homozygous TT genotype cases were in this age group, youngest being 25 years age. Co-occurrence of homozygous methylenetetrahydrofolate reductase (MTHFR) TT and angiotensin-converting enzyme (ACE) D/D genotypes yielded a highly significant moderate risk of leukoaraiosis (ischemic white matter demyelination),[10] in a Hungarian study. In present study, no significant correlation was found between the studied factors (hyperhomocysteinemia, TT and CT genotypes) and single vs recurrent stroke. Larger studies may resolve this issue. The effect of genetic polymorphism can be influenced by environmental factors. Synergistic effects between the ACE D/D and MTHFR TT genotypes and drinking or smoking,[11] has been found. MTHFR genotype could also be an important risk factor with low folic acid intake. In present study, 15.6% patients were folate deficient, including two of three homozygous cases. In previous study,[5] 32% of CAD cases with hyper-homocysteinemia were folate deficient. It is thus suggested that in adult patients with homozygous MTHFR C677T polymorphism, higher doses of folic acid/B-complex could overcome defect due to TT genotype and may serve as a feasible option for stroke prevention. Acknowledgements We sincerely thank Mr. Suresh Kumar for technical support and residents in Neurology for help in conducting the relevant studies.References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06010t1.jpg] [ni06010t2.jpg] |
| |||||||||

{kind=link}
{kind=link}