 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
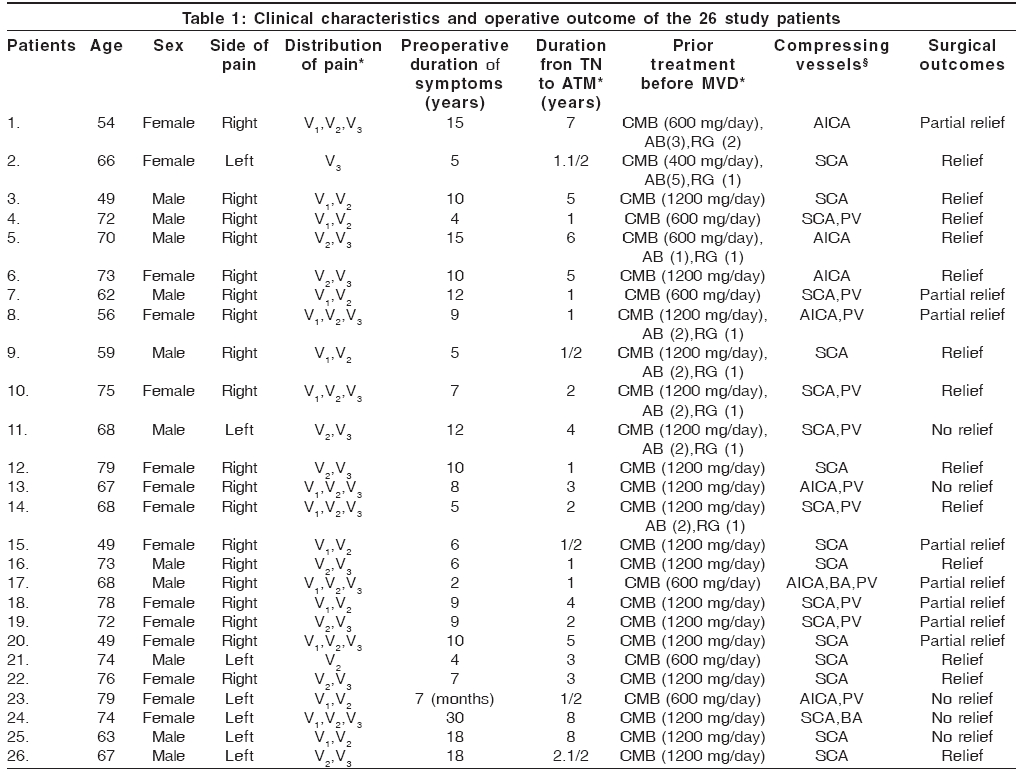
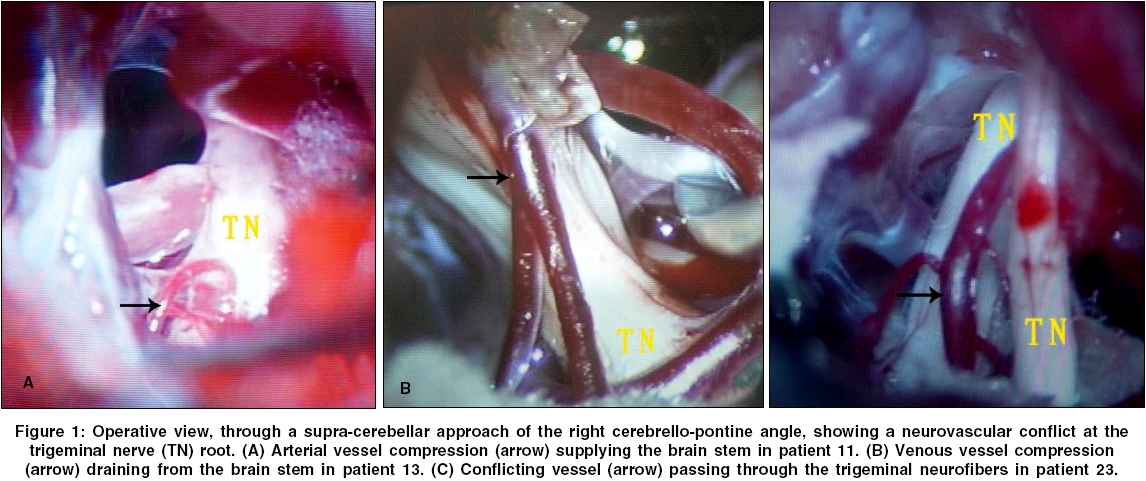
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 53-56 Original Article Treatment of atypical trigeminal neuralgia with microvascular decompression Hai Jian, Li Shi-Ting, Pan Qing-Gang Department of Neurosurgery, Tongji Hospital, Tongji University, Shanghai - 200065 Code Number: ni06013 Related article: ni06014 Abstract Aim: To explore the methods for achieving pain relief in patients with atypical trigeminal neuralgia (TN) using microvascular decompression (MVD).Study Design and Settings: Retrospective study of 26 patients treated during the years 2000 to 2004. Materials and Methods: Twenty-six patients in whom vascular compression of the trigeminal nerve was identified by high definition magnetic resonance tomographic angiography (MRTA) were treated with MVD for atypical TN in our department. Clinical presentations, surgical findings and clinical outcomes were analyzed retrospectively. Results: In this study, single trigeminal division was involved in only 2 patients (8%) and two or three divisions in the other 24 patients (92%). Of prime importance is the fact that in 46.2% of the patients, several conflicting vessels were found in association. Location of the conflicts around the circumference of the trigeminal root was supero-medial to the root in 53.5%, supero-lateral in 30.8% and inferior in 15.7%. MVD for atypical TN resulted in complete pain relief in 50% of the patients with complete decompression, partial pain relief in 30.8% and poor pain relief or pain recurrence in 19.2% of the patients without complete decompression postoperatively. Conclusions: Complete decompression of the entire trigeminal root plays an important role in achieving pain relief in patients with atypical TN with MVD. Keywords: Atypical trigeminal neuralgia, microvascular decompression, magnetic resonance imaging, neurovascular compression. Introduction Trigeminal neuralgia (TN) is one of the most common causes of facial pain. A typical TN is characterized by transient episodes of lancinating pain in the trigeminal distribution, often precipitated by mild mechanical irritation from activities such as brushing the teeth or chewing associated with trigger zones.[1] Since Dandy theorized that vascular compression of the trigeminal nerve is responsible for TN, microvascular decompression (MVD) has been widely used with favorable outcomes.[2],[3] Although the immediate success rates of MVD for the treatment of typical TN is more than 90%, but the incidence of pain relief in patients with atypical TN has been reported to only about 50%.[4],[5],[6] Atypical TN may share a different clinical characteristics from typical TN. In order to explore the methods for achieving pain relief in patients with atypical TN using MVD, we analyzed clinical presentations, surgical findings and clinical outcomes in 26 patients with atypical TN retrospectively. Some key points during the procedures of MVD should be considered preoperatively and intraoperatively. Materials and Methods Between 2000 and 2004, 26 patients with atypical TN referred to our department performed by MVD. On admission, each patient′s history and clinical condition were checked and recorded in details by the same neurosurgeon, including age, sex, symptom, trigger zone, prior treatment, duration and characteristics of facial pain. All the information in this study were retrieved and analyzed retrospectively with ethical clearance from the review board in our hospital and informed consents from patients. Of these cases, mean age was 65 years (range: 49 to 79 years). 58% were females and 42% were males. 69% had pain on the right side and 31% on the left. V 2 or V 3 division was affected in 8% and more than one division in 92% (V 1,2 distribution in 8 patients, V 2,3 in 8 patients and V 1, 2, 3 in 8 patients). Duration of pain before MVD was 9.1 years on average (range: 7months to 30 years). The clinical characteristics of the 26 patients are shown in [Table - 1]. In this series, all patients were resistant to prolonged and high doses of carbamazapine. 8 (30%) patients had received other surgical treatment such as alcohol block (1 to 5 times) and radiofrequency gangliolysis (1 to 2 times) before MVD. Every patient with atypical TN should take magnetic resonance tomographic angiography (MRTA) examination preoperatively. MRTA is an extremely sensitive and specific method for demonstrating vascular compression in trigeminal nerve.[7] Once vascular compression of the trigeminal nerve was identified, the procedure of MVD may be advocated. In the same period, two patients with atypical TN without definite neurovascular compression by MRTA were excluded from this study [Figure - 1]. Atypical TN denotes a syndrome in which patients describe unilateral pain which, although it is in a trigeminal distribution, is more burning or aching in nature without definite trigger zone. This discomfort may be continuous or nearly continuous and rarely responds to any of the aforementioned medications.[4],[5] Many patients suffered from atypical TN even presented with facial numbness associated with sensory loss. The technique that we used for posterior fossa exploration was the same as is currently performed through a supracerebellar-infratentorial approach using a small (1.5-3 cm) retromastoid craniectomy. This allowed one to gain access to the entire trigeminal root, from its exit from Meckel′s cave to the trigeminal root entry zone (REZ). Technical details have been described in previous publication.[3] Under the microscope it was possible to look at the entire trigeminal root, from the Meckel′s cave to the REZ at the pons. Various types of conflicting vessels and location of the conflicts around the circumference of the root were observed specially. Only the main conflicting vessel if several in the same patient, was considered for the study. For MVD, Teflon sponge was used in all patients. Before the end of operation, we examined and recorded the final decompression degree as complete or incomplete. Complete decompression denotes that all offending vessels were dissected and moved away from trigeminal nerve and Teflon was insert enough to keep the vessels off the nerve. Incomplete decompression was usually resulted from the followings: (1) The offending vessel was petrosal vein or its branches and the adhesion could not be dissected from trigeminal nerve. (2) The offending vessel located in the REZ and gave off several penetrating arteries into the brain stem. Teflon sponge could not be inserted enough into the limited interspace. (3) The offending artery passed through trigeminal neurofibers. The outcome of the intervention was graded as follows: Complete relief of symptoms, or excellent outcome, was defined as the absence of facial pain; Partial relief, or good outcome, was defined as a 75 percent reduction in pain as assessed by the patient with low doses of medication; Poor outcome was defined as a less than 25 percent in pain compared with the preoperative level.[3] The mean follow-up was 2.8 years, and the follow-up periods ranged from 3 mouths to 4 years after the MVD procedure. Results In this study, all patients initially began with the symptoms of typical TN. As the disease progressed, the patients gradually lacked the typical characteristics of TN and presented with atypical TN syndromes. The mean duration from typical TN to atypical TN was about 3 years (range: 6 months to 8 years) as shown in [Table - 1]. Satisfactory images of the trigeminal nerves and posterior fossa vessels were obtained with MRTA in all cases. Arterial vessel compression can be identified clearly. However, vascular types and venous vessels can not be assessed adequately. Owing to the demonstration of neurovascular compression by MRTA before operation, vascular conflict was found in all patients. In this series, one (or several) conflicting vessel(s) were identified: the superior cerebellar artery (alone or in association with other conflicting vessels) in 73.1% of the patients, the anterior inferior cerebellar artery in 26.9%, a vein embedded in the nerve in 42.3%, the basilar artery in 7.7%. Of prime importance is the fact that in 46.2% of the patients, several conflicting vessels were found in association. As for the location of the conflicts around circumference of the trigeminal root, only the main conflicting vessel if several in the same patient was considered for the study. Location was supero-medial to the root in 53.5%, supero-lateral in 30.8% and inferior in 15.7%. MVD for atypical TN resulted in complete pain relief in 50% of the patients with complete decompression, partial pain relief in 30.8% and poor pain relief or pain recurrence in 19.2% of the patients without complete decompression postoperatively. Significant pain relief after MVD was achieved in 80.8% of all the patients. It is difficult to carry out complete neurovascular decompression in some conditions, including venous vessel compression, arterial vessel compression supplying the brain stem, medial vessel compression or conflicting vessel passing through the trigeminal neurofibers. Adequate decompression of arterial or venous vessels associated with the brain stem may result in severe nervous dysfunction. The surgical outcomes of the 26 patients are shown in [Table - 1]. The occurrence of complications related to MVD was very low. In this series, only two patients suffered from transient facial paresis and hearing disturbance which resolved 2 to 4 months after operation. Discussion TN is a well-known and relatively common disorder, which, in its classic description, fulfills several clinical criteria.[8] First, the pain is localized to one or more branches of the trigeminal nerve. The pain has a sharp, shooting, lanciating, "electric shock"-like character and occurs as a brief episode or attack, lasting several seconds, with pain-free intervals between attacks. The attacks are initiated by stimulation of so-called "trigger zones" or they may start spontaneously without obvious provocation. In this study, all patients initially began with the symptoms of typical TN. However, the patients gradually lacked the typical characteristics of TN and presented with atypical TN syndromes with time. Typical and atypical TN may present two different kinds of pathological process in the same disease.[9] Current treatment usually begins with medication such as carbamazepine or phenytoin, which frequently provides relief from symptoms. Unfortunately, the pain relief may decrease over time, and side effects may necessitate discontinuation of the medication. Many patients eventually require an operation for pain relief. Several percutaneous operative treatment for TN are in current use, including alcohol block, radiofrequency gangliolysis, glycerol rhizotomy.[5] However, these procedures all create trigeminal nerve lesion, occasionally producing facial anesthesia or keratitis. In 1934, Dandy proposed the neurovascular compression theory accounting for TN.[2] Since that time, Gardner and Miklos are credited for being first to decompress a trigeminal nerve as a treatment for TN.[10] Jannetta further explored and popularized MVD as an effective treatment for TN.[11] Although MVD for typical TN resulted in significant pain relief in more than 90% of patients, the incidence of pain relief in patients with atypical TN has been reported to only about 50%.[4],[5],[6] It remains unknown how to increase the rates of pain relief in patients with atypical TN. In this study, neurovascular compression may also account for the occurrence of atypical TN and significant pain relief after MVD was achieved in 80.8% of all the patients. Through intraoperative observation, we found that several conflicting vessels compressed the entire trigeminal root in association. Jannetta hypothesized that the compression must be at the REZ of the trigeminal nerve to cause TN.[12] However, some authors suggested that the compression can occur at any point along the cranial nerve and not only at REZ. In addition, there is considerable evidence that any vascular contact (artery or vein) can cause symptoms.[13],[14] Our results also showed that complete decompression along the entire trigeminal root is very important for pain relief. Missing any offending vessels might lead to immediate surgical failure or recurrence. In order to achieve pain relief in patients with atypical TN by MVD, we think that it is essential to analyze the clinical characteristics carefully and confirm the presence of conflicting vessels using MRTA preoperatively. The topography of facial pain may be related to the location of the conflicting vessels around the circumference of the trigeminal root.[15] To our knowledge, it is difficult to carry out complete neurovascular decompression in some conditions, including venous vessel compression, arterial vessel compression supplying the brain stem, medial vessel compression or conflicting vessel passing through the trigeminal nerve, which may account for poor pain relief or pain recurrence in patients with atypical TN after MVD. Experience from this study, early MVD should be considered as the best treatment choice for patients with atypical TN, especially in whom the duration of symptom lasts no longer than 3 years and neurovascular compression has been confirmed by regular MRTA. For the recurrent case after MVD, reoperation may be advocated if we think that complete decompression has not been achieved during the first procedure. For the patients with partial pain relief postoperatively, continuous drug treatment may be an adjuvant way. In addition, some patients with pain recurrence or no pain relief may also resort to the other minimally invasive treatment such as stereotactic radiosurgery. In conclusion, complete decompression of the entire trigeminal root play an important role in achieving pain relief in patients with atypical TN by MVD. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06013f1.jpg] [ni06013t1.jpg] |
| |||||||||

{kind=link}
{kind=link}