 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
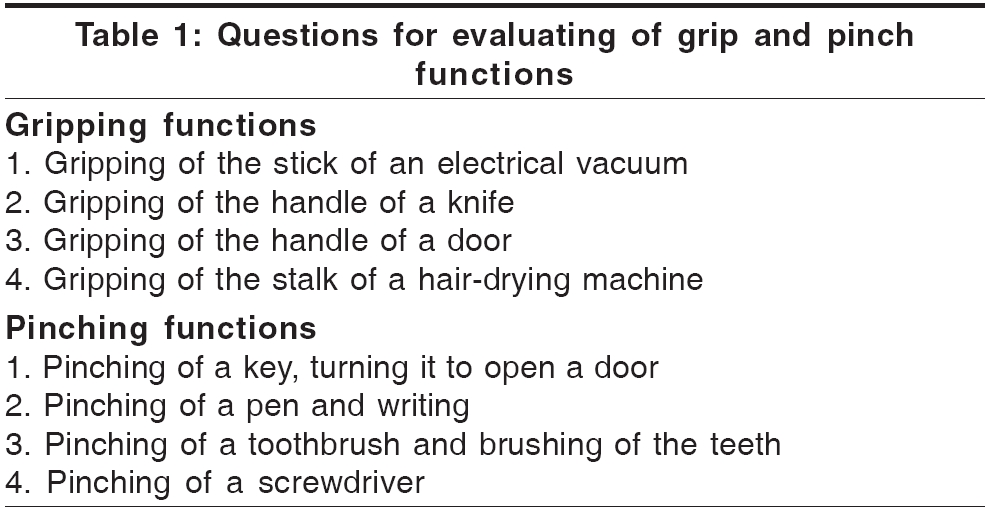
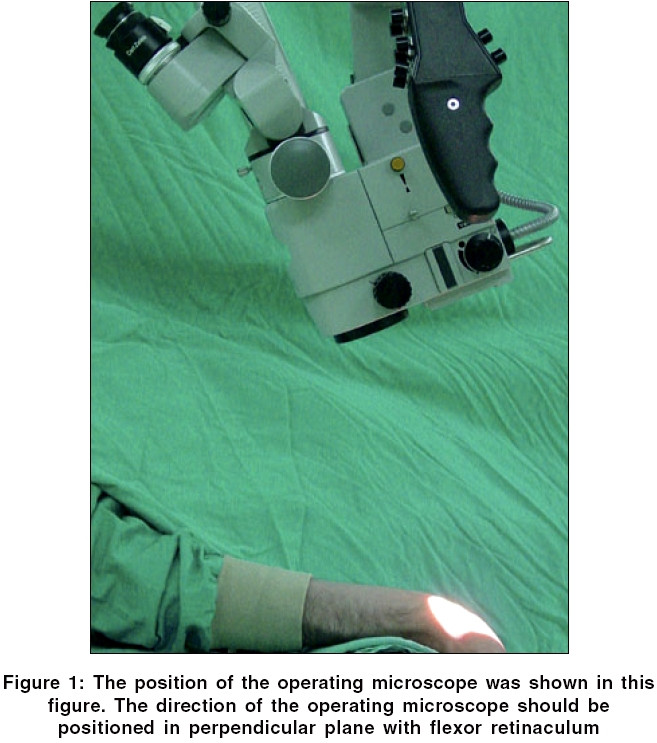
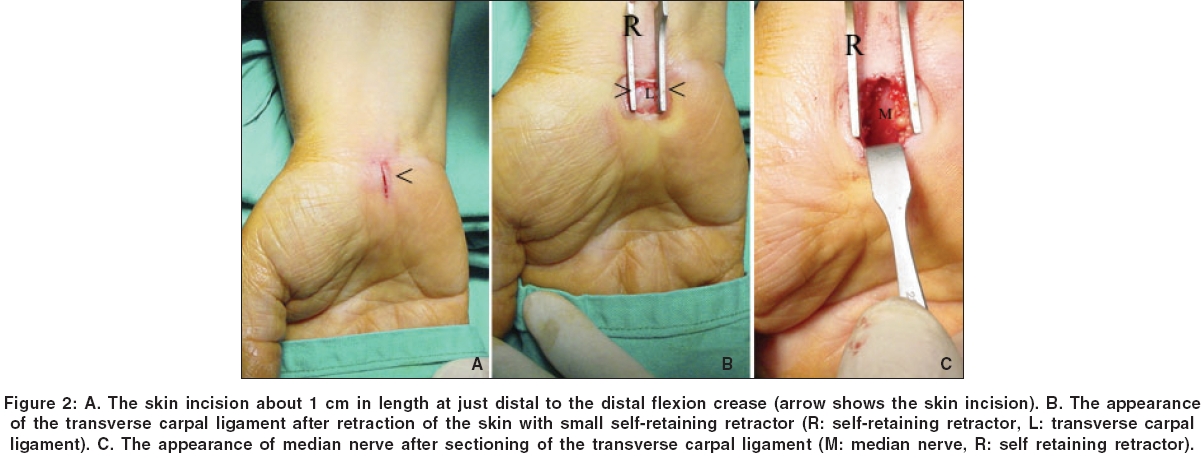
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 64-67 Original Article Microsurgical open mini uniskin incision technique in the surgical treatment of carpal tunnel syndrome Keramettin Aydin, Cengiz Cokluk, Nilgun Cengiz, Ayhan Bilgici Department of Neurosurgery, Medical Faculty, Ondokuzmayis University, Samsun Code Number: ni06017 Abstract Background: Patients who undergo carpal tunnel surgery sometimes complain of the restriction of the grip and pinch function, palmar tenderness, cosmetic problems, and scar formation at the site of the incision.Aims: We used a modified mini uni-skin incision with appropriate hand position for microscopic view in the surgical treatment of carpal tunnel syndrome to prevent cosmetic problems related with scar formation after surgery. Settings and Design: In this study we used two different skin incision techniques; mini uni-skin incision and standard incision. In mini uni-skin incision technique the hands were positioned in a way that the wrist are hyperextended. A small skin incision one cm long was done from the inferior flexion crease towards the point between the thirth and fourth fingers. Materials and Methods: Standard incision and mini uni-skin incision were compared according to their cosmetic result, grip and pinch function, palmar tenderness, and painful scar formation. Statistical analysis: Student -t test was used for this study. Results: 56 (43%) patients were operated with mini uni-skin incision, and 73 (57%) cases were operated with standard incision. The scores of grip, pinch and cosmetic results were better in the patients who were operated with mini uni-skin incision technique from those of standard incision. Conclusion: In this clinical study we used a modified skin incision (mini uni-skin incision) technique in the surgical treatment of carpal tunnel surgery. Our results revealed that mini uni-skin incision is superior from the standard incision. Keywords: Mini open uniskin incision, open median nerve release, carpal tunnel syndrome. Introduction Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy, accounting for more than 200,000 surgical procedures per year in the United States. Approximately 1% of population is affected by carpal tunnel syndrome.[1], [2] Common clinical presentations include painful paresthesias or burning pain in the lateral half of the hand and the radial three fingers.[1] History, physical examination, electromyography, and nerve conduction velocity measurements are essential for the diagnosis.[3] Open carpal tunnel release has been widely used as a surgical alternative for patients who are resistant to the conservative treatments. However, although its effectiveness has been recognized, open carpal tunnel release has been associated with problems such as hypertrophic scarring, scar tenderness and delayed rehabilitation.[4],[5] Various limited skin incisions and endoscopic techniques have been proposed as a minimally invasive and effective for preventing of the excessive scar formation and the achieving of a better cosmetic results.[1],[3], [6],[7],[8],[9] In this clinical study, we described a modified surgical technique (mini-open uni-skin incision), and compared it with the standard incision according to the capability of grip and pinch function, cosmetic results, palmar tenderness and painful scar formation. Materials and Methods Local ethical committee (Ondokuzmayis University, Medical Faculty, Local Ethical Committee) approved this clinical study. Before operation all patients and/or their family were informed about the type of the operation. This retrospective study included 129 female right hands with carpal tunnel syndrome underwent microsurgical intervention for median nerve release using mini-uniskin incision and standard incision between 2001 and 2005. The diagnosis was made from the patient′s history, physical examination, the results of electromyographic studies, and nerve conduction velocities in all cases. Patients with left and bilateral carpal tunnel syndrome were not included to the study. Follow up examinations of the cases were made 20, 60, and 90 days after the operation. A dermatologist and a doctor of physical medicine examined all patients in the aspect of cosmetic outcome, grip and pinch functions. The patients were examined in the aspect of grip and pinch function, palmar tenderness, and painful scar formation. We used some simple questions selected from the daily activities in the evaluation of grip and pinch functions. [Table - 1] showed the questions for evaluating of these function. Grip and pinch function, palmar tenderness, and scar formation were clinically graded four level as poor, moderate, good, and excellent in according to patient′s description and physical examination. Numerical values were given for each levels, 0 for poor, 1 point for moderate, 2 point for good, and 3 point for excellent. Student -t test was used for statistical analysis. Surgical technique Standart incision technique Mini uni-skin incision technique A mini skin retractor was used to retract the incisioned skin [Figure - 2]B. The subcutaneous fat tissue was dissected laterally. 15 no surgical blade was used to open proximal part of the ligament. After this maneuver, the ligament was cut with a micro scissors. Our experience showed us that the maneuver of the hyperextension of the hand provide a good surgical route with the depletion of the median nerve and the tendons of the fingers to the posterior bony wall of the tunnel. Because of this, the sectioning of ligament with scissor is safe and reliable. The surgical area was then irrigated with sterile saline solution and homeostasis was obtained with bipolar coagulation. The sectioning of the ligament was checked along the carpal tunnel, and the median nerve was inspected [Figure - 2]C. The skin was sutured with interrupted 4-0 nylon sutures without subcutaneous suture. The mean operating time was 30-45 minutes. The skin sutures were removed 10 days after the operation. Results The present study includes 129 female wrists with carpal tunnel syndrome aged between 36-72 years old. All patients had the evidence of median nerve entrapment at the wrist in the electromyographic studies and nerve conduction velocities. 56 (43%) of them were operated with mini uni-skin incision, and remaining 73 (57%) were operated with standard incision. The mean follow up period was 2 years. There was no reoperation, skin infection, and palmar cutaneous branch injury in all groups. [Table - 2] shows the scores of grip and pinch function, palmar tenderness, cosmetic results, and postoperative course for patients operated with both methods. The scores of grip, pinch and cosmetic results were better in the patients who were operated on with mini uni-skin incision technique from those of standard incision in the ratio of 26%, 17%, and 54% respectively. Palmar tenderness was lower in patients operated on with mini uni-skin from those of standard incision. The differences between these two groups are statistically significant ( P < 0.01). Discussion If a surgery is necessary for median nerve decompression, the surgical technique should be less traumatic and minimally invasive for both of median nerve and palmar skin to prevent the postoperative sequels and achieve a good postoperative course without persistent symptoms. Damage of the palmar cutaneous branch of the median nerve, reflex sympathetic dystrophy, hypertrophic scar formation, scar sensitivity, palmar hematoma, bowstringing of the flexor tendons, double crush, and adherence of the flexor tendons had been reported as the causes of persistent symptoms after median nerve release.[11],[12],[13],[14] The most common and less serious sequels of carpal tunnel surgery related with skin incision are hypertrophic scar formation, sensitive scar, tenderness and cosmetic dissatisfaction.[1], [2] The incidence of these types of sequels has been reported in some series at 24%.[1] Standard open procedures with different type skin incisions; endoscopic techniques have been described for surgical division of the transverse carpal ligament.[3],[6],[7],[8],[9],[11],[15],[16],[17],[18],[19] The aim of this clinical study was to use a shorter skin incision to reduce the number of sequelae of the carpal tunnel surgery related with skin incision and compare this with the results of the standard skin incision technique. Open mini uni-skin incision is different from standard technique in terms of localisation and length of the incision, and position of the hand under the operative microscope. We identified a triangle on the proximal part of the palm in the localization of the skin incision. The skin is relatively thin, and biomechanically less movable in this triangle in comparison with other parts of the palm. This incision also facilitates the release of proximal transverse carpal ligament. We standardized our patient population by selection of right-handed women. Questions for evaluating of the grip and pinch function includes some functions commonly used by women in daily activities. The patients described the capability of their hands during making of these activities such as poor, moderate, good, and excellent. The mean scores of grip function were found better in the ratio of 26% in the patients who were operated with mini uni-skin incision technique. The scores of pinch function were also better in the ratio of 17% in the patients operated with mini uni-skin incision. The clinical data from the present series suggested that cosmetic results of mini uni-skin incision were superior from those of standard skin incision. Sensitive scar formation and tenderness were also less in mini uni-skin incision group from those of standard incision. The differences between these two groups were statistically significant. Although in large series, cosmetic problems originated from excessive scar formation seems relatively uncommon problem after carpal tunnel surgery. But it is clear that palmar skin surface lost their biomechanical movements and elasticity after surgery even in normal wound healing process. The limited skin incision occupies small area on the palmar surface of the hand. This provides more movement capability, elasticity and better appearance to the skin surface. Conclusion The mini uni-skin incision technique for median nerve release can be used in the surgical treatment of carpal tunnel syndrome to achieve a better palmar appearance. Our clinical data revealed that this technique is superior to standard incision in the aspect of grip and pinch function, and cosmetic results. Our observation revealed that the patients operated with mini uni-skin incision technique have an easier postoperative course in comparison with standard incision.References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06017t1.jpg] [ni06017f1.jpg] [ni06017t2.jpg] [ni06017f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}