
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 54, Num. 1, 2006, pp. 68-72
|
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 68-72
Original Article
Carotid artery stenting: Results and long-term follow-up
Gupta AK, Purkayastha S, Kapilamoorthy TR, Nair MD, Krishnamoorthy T, Rupa S, Kesavadas C, Bodhey NK, Thomas B
Departments of Radiology, Sree Chitra Tirunal Institute of Medical Sciences and Technology, Trivandrum, Kerala
Correspondence Address:Department of Radiology, Sree Chitra Tirunal
Institute of Medical Sciences and Technology, Trivandrum, gupta@sctimst.ac.in
Code Number: ni06018
Abstract Background and Purpose: The role of carotid artery stenting (CAS) as an alternative to carotid endarterectomy in the treatment of for symptomatic carotid artery stenosis is investigated.
Materials and Methods: Forty-seven patients underwent CAS over 10-year period. Forty-nine vessels were treated. Stenosis quantification was done using North American symptomatic carotid endarterectomy trial method. The mean follow-up period by clinical and Duplex examination ranged is 5.6 years.
Results: The technical success rate was 100%. There were four deaths (8.1%) and two (4.1%) minor strokes within thirty days of procedure. There was no major strokes. All patients with minor stroke achieved complete recovery at 1-month follow up. Two deaths occurred probably due to hyperperfusion syndrome (HS) and two due to cardiac arrest.
Conclusion: CAS is an effective treatment modality of symptomatic
carotid artery disease but should be carefully done in high-risk groups
having severe medical ailments and those having severe bilateral stenosis
of the carotid arteries.
Keywords: Carotid artery stenting; interventional radiology; stroke.
Surgical carotid endarterectomy (CEA) is currently the accepted standard mode of treatment for revascularization of extracranial carotid occlusive disease.[1],[2],[3],[4],[5] Carotid artery stenting (CAS) is currently being investigated as an alternative treatment to CEA.[6],[7],[8],[9],[10],[11] The purpose of the present study is to analyze our experience, determine the therapeutic benefits of CAS in preventing stroke and to describe the technical details of the procedure.
Materials and Methods
CAS was performed on 47 patients (35 males and 12 females) at our institution
between January 1995 and June 2005. These cases were analyzed retrospectively.
To be considered suitable for stenting, symptomatic patients had at least
50% stenosis and asymptomatic patients had at least 70% diameter
narrowing. This is as per the criteria laid down by North American symptomatic
carotid endarterectomy trial (NASCET).[4],[5],[12] Forty-five patients had recurrent transient ischemic attacks or stroke ipsilateral to the side of carotid stenosis, which was resistant to medical treatment. Two patients had high-grade asymptomatic carotid stenosis.
Clinical protocol
Carotid Doppler study, CT or MR imaging, routine blood investigations,
cardiological and neurological evaluation was performed by a team of
consensual staff. National Institutes of Health Stroke Scale (NIHSS)
was recorded before the procedure and at 24 h, 30 days and subsequently
at 3 month interval. Antiplatelet therapy was started 2-4 days before
the procedure. Follow-up Doppler study was obtained at first month and
then every 3 months.
Definitions of clinical terms
Technical success was defined as the ability to access the carotid
artery and successfully stent the lesion with residual stenosis of no
more than 20%. Study end points were defined as an occurrence within 30 days of minor stroke, major stroke, death, or myocardial infarction (MI). Myocardial infarction was assessed clinically and ECG evidence of ischaemia. Minor stroke was defined as an increase in the NIHSS score of less than 3, with complete resolution or no significant disability at 30 days. Major stroke was defined as an increase in the NIHSS score of 3 or more, with significant disability at 30 days. Severe coronary artery disease was defined as angiographic evidence of triple vessel disease with stenosis of more than 70%.
Technique of carotid artery angioplasty and stenting
The procedure was performed under sedation and local anesthesia.
A baseline activated clotting time was obtained. Preprocedure diagnostic
angiography of neck vessels and intracranial circulation was performed.
Stenosis was quantified according to NASCET criteria. The patients activated
clotting time was kept 2-2.5 times the baseline. Initially stenosis was
traversed under digital road map guidance with a 300 cm, 0.014 in. exchange-length
guide wire. Protection devices were used in six patients. If patient
affords, we intend to use protection devices routinely. After predilation,
the stent was placed across the lesion referenced by bony landmarks and
postprocedure angiograms were obtained. Postdeployment angioplasty was
done in cases where the stent opening was thought to be inadequate after
deployment. Postprocedure mean arterial pressure was kept 10-20% below
baseline to prevent cerebral reperfusion injury.
Results
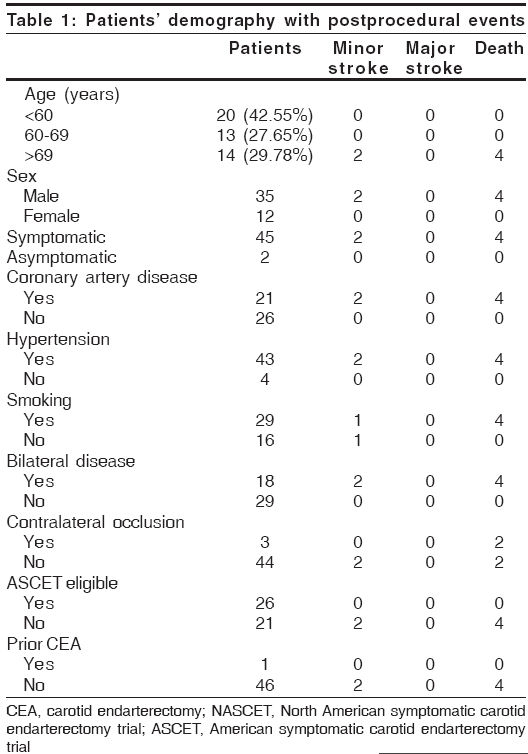
Demographic, clinical and morphological characteristics
A total of 49 vessels were treated during 48 procedures [Table - 1].
The mean age of the patients was 61.2 years. Significant coronary artery
disease (angiographically proved triple vessel disease with stenosis greater
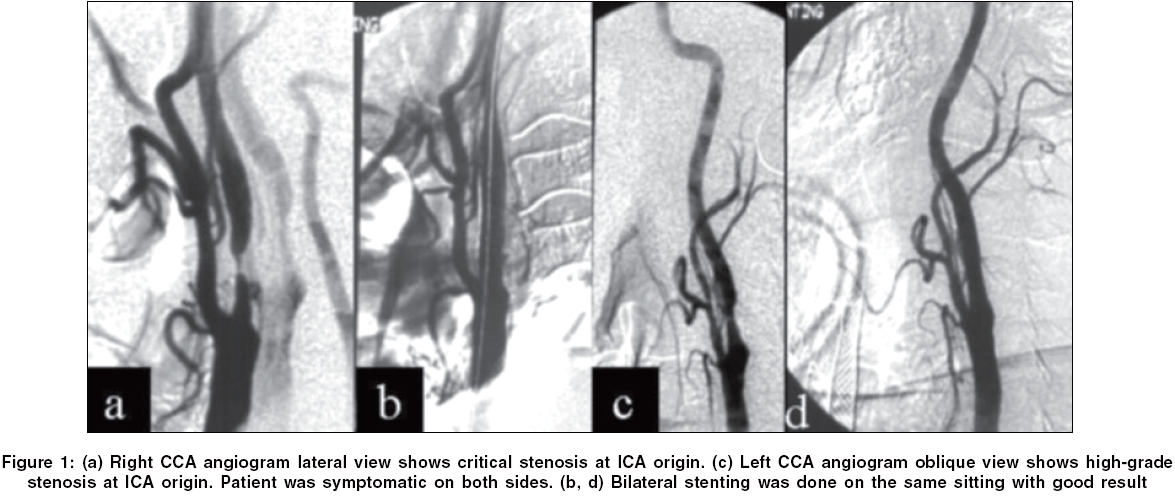
then 70%) was present in 21 patients (44.68%). Significant disease in both carotid arteries was present in 18 patients (38.29%) and contralateral carotid artery occlusion was present in 3 (6.38%) patients. Lesion severity of> 90% was present in 17 vessels (34.69%). A bilateral carotid procedure was undertaken in two patients (4.25%) [Figure - 1]. These two patients were symptomatic on both sides with stenosis> 70% (NASCET criteria). Of the 45 patients (95.74%) with symptomatic carotid stenosis in this series who met the angiographic criteria, only 26 (57.7%) would have been eligible for inclusion in NASCET. Protection devices were used in six patients (six procedures). Wall stents (Boston Scientific Corporation, USA) were used in all. The length and the diameter of the stents ranged from 40-80 to 6-8 mm, respectively. Technical success was achieved in 100% of
procedures.
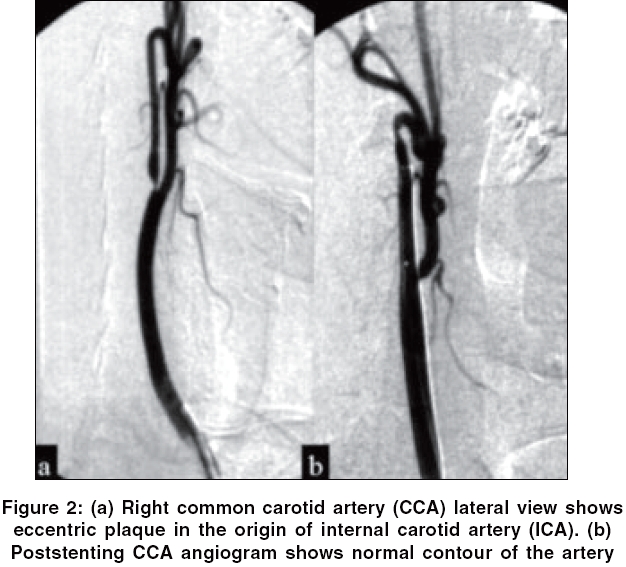
Angiographic characteristics before and after stent placement
Angiographic morphology indicated 34 concentric lesions of ICA and
15 eccentric plaques [Figure - 2]. The lengths of the stenoses were 7-36
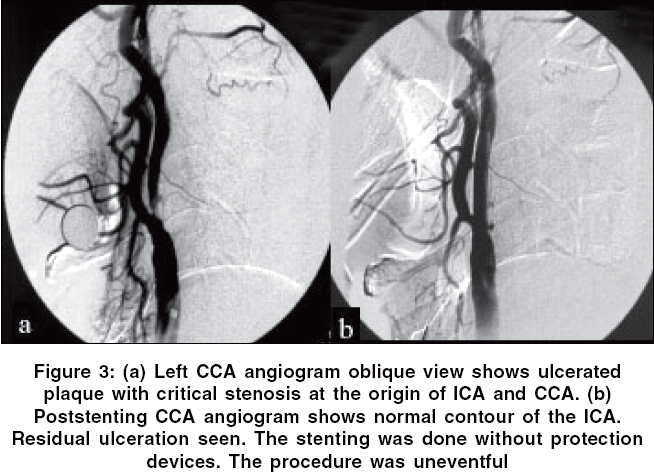
mm (mean: 15 mm). Twenty-nine plaques showed the typical niches of ulcerations.
Calcification was seen in 15 lesions. Stent implantation reduced the mean
percentage of stenosis (according to the NASCET criteria) from 83.8 to
6.3%, which is highly significant ( P < 0.001, Wilcoxon test). In one case there was a residual small ulceration after the stent placement [Figure - 3]. Due to the small size of the ulcer,it is being observed on antiplatelet therapy. In this patient at 1-month follow up no ulcer crater was visible on Duplex and the patient remained asymptomatic till his last follow up at 3 years. Wallstent implantation induced kinking of the ICA above the distal end of the stent in two cases. The kinks were associated with moderate (5-10%)
stenoses. This was due to severe tortuosity of the vessel, however, there
was no flow limitation. Due to this reason a second stent was not put to
rectify the kink.
Sonographic characteristics before and after stent placement
All stenoses were 70% or greater, according to Doppler criteria
(acoustic evaluation, peak systolic velocity and duplex measurement of
local luminal narrowing). Sonographic plaque morphology confirmed 16 echolucent
smooth plaques, six echodense plaques and 26 lesions of mixed echodensity
with ulcerations. Duplex sonograms depicted an irregular surface in 26
plaques and showed coincident findings in 26 of 29 angiographically proved
irregularities. Sonograms depicted three further plaques that were incompletely
covered by the proximal end of the stent . As the plaques were thin
and were situated in mid-CCA, second stents were not put in them. High-resolution
sonograms (obtained in power mode) depicted two cases of ulcer niche that
persisted immediately after stent placement but no ulcer was seen at 1-month
follow up and the patients remained asymptomatic. Mild in-stent intimal
thickening was noted in three patients on follow-up Doppler study at 6
months, but they were stable up to latest follow up at 48 months.
Procedural outcomes
Cinical characteristics and procedural outcome of the patients are
given in [Table - 1]. A total of two neurological events were noted within
30 days of stenting in 49 carotid arteries. These included two minor strokes
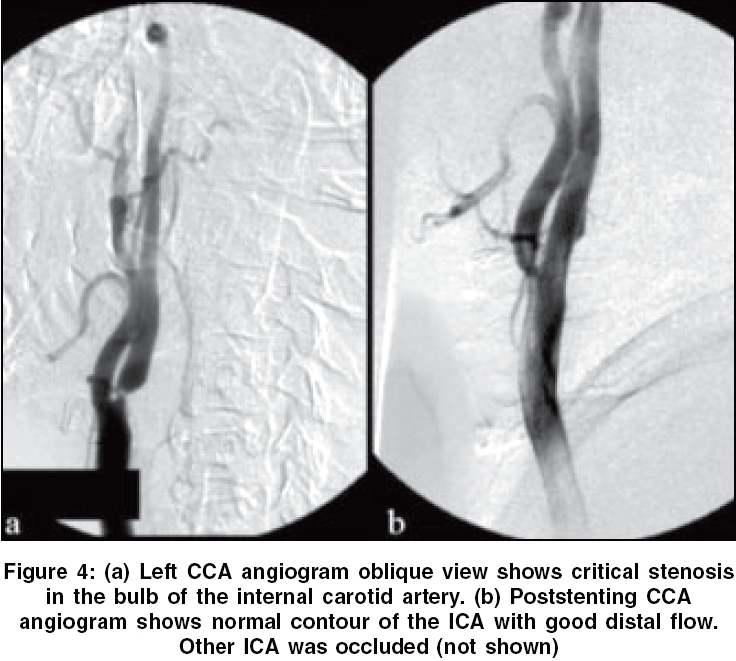
after the procedure (4.1%) and they recovered completely. These were thought to be of embolic origin and happened in patients where no protection devices were used. There were four deaths within 7 days of procedure, two related to hyperperfusion and two due to cardiac arrest. One patient with bilateral carotid stenoses and the other with one side carotid occlusion and other side having 98% stenosis
had hyperperfusion syndrome despite strictly controlling the blood pressure
below baseline [Figure - 4]. One patient died within 24 h and the other
within 4 days of the procedure. The third patient having prior history
of MI and had undergone bilateral stenting died of cardiac arrest after
2 days of the procedure. The fourth patient had severe triple vessel coronary
artery disease and one side carotid occlusion also died of cardiac arrest.
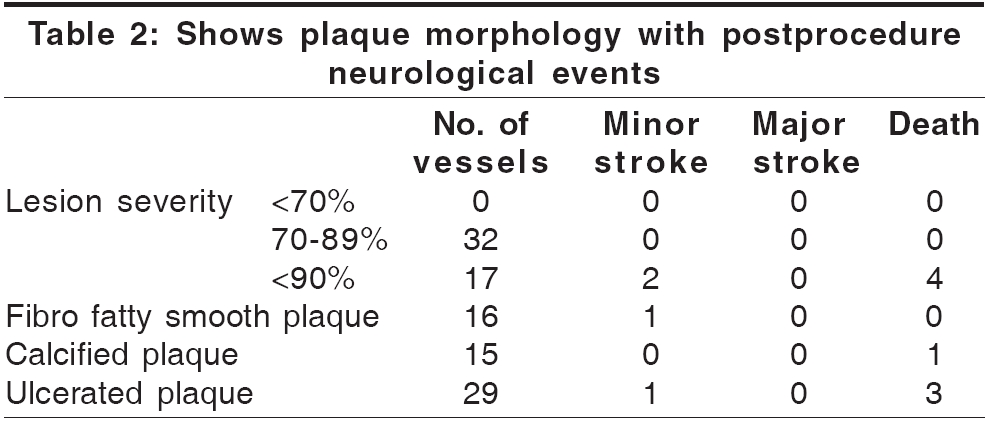
The relation between plaque morphology and procedural outcome are given
in [Table - 2]. Most of the complications were seen in high-grade stenosis
with ulcerated plaques ( P = 0.011, Fisher′s exact test).
Predictors of neurological events
All the complications are seen with patients older than 70 years of
age ( P =
0.006, Fisher′s exact test). Presence of bilateral carotid lesions
( P = 0.017), contralateral carotid occlusion ( P = 0.016)
and severe coronary artery disease ( P =
0.034) had significant influence on risk of stroke and death. Lesion severity
(>70%) was also associated with the risk of stroke and death ( P =
0.011, Fisher′s exact test).
Clinical outcome and follow up
The follow-up ranged from 6 months to 9 years. One minor ipsilateral
stroke (2.04%) occurred 15 months after stent placement in a 78-year-old patient and she had total recovery with patent stent. One patient stopped antiplatelet medication 3 years after the procedure and she had a fainting attack. Her Doppler showed total stent occlusion, but she was neurologically normal. On follow-up Doppler study all the patient stents were covered well by intima and were patent. Only two vessels showed (4.08%) mild (10-15%)
restenosis inside the stent with any flow restriction and neurological
event. All other patients were symptom free on last follow up (mean 5.6
years).
Discussion
Percutaneous transluminal balloon angioplasty was first reported in 1980 and since then a number of reports are available in the literature detailing high success rate of the procedure.[13],[14],[15],[16],[17],[18] The concept for stent placement has come from successful trials in the coronary arteries.[15],[16]
Yadav
et al. reported their result in 77% of NASCET ineligible patients.[9] In
our series 57.77% of patients did not fulfill NASCET inclusion
criteria and all our complications were encountered in this group of
patients.
Stent oversizing and cerebral protection is theoretically advantageous
in preventing distal embolism and in reducing tissue prolapse and is
associated with a lower rate of restenosis.[19],[20],[21],[22] So,
we choose stents 3-5 mm larger then the vessel diameter to avoid these
problems. Theron et al. reported good result with distal balloon protection
and depends on the emboli size.[6],[23],[24],[25] We
have not encountered any embolic episode since we started using the protection
devices.
Large series of extracranial carotid angioplasty and stenting have
revealed the incidence of stroke and death to be in the range of 3.6-7.9%.[9],[26] In
the present series the combined stroke and mortality rate is 12% and
the patients had either bilateral critical carotid stenoses or unilateral
carotid occlusion with contralateral critical stenosis and the patients
had a prior coronary artery bypass grafting for critical triple vessel
disease. This high rate of stroke is also due to lack of usage of protection
devices in most of our cases. Recent report from the data of SAPPHIRE trial
clearly showed the advantages of protection devices in preventing the periprocedural
stroke in CAS.[27] Postprocedural
hyperperfusion intracerebral hemorrhage been
reported as a rare complication of CEA and stenting, with an incidence
upto 5%. [28],[29],[30],[31],[32],[33] We
have seen two deaths (4.2%) related to HS. Severe (>90%)
ipsilateral stenosis, contralateral occlusion, increased age, impaired
collateral blood flow or an incomplete circle of Willis, perioperative
and postoperative hypertension and use of antiplatelet agents or other
anticoagulants are risk factors for the development of postCEA intracerebral
hemorrhage.[34],[35],[36] Our
experience suggests that bilateral procedures should not be done in the
same sitting to reduce the chances of HS. When this treatment is required
for such patients, extreme postprocedural care must be taken. Protection
devices appear to play a role in avoiding this problem.[37],[38]
Lack of cerebral protection, poor patient selection and the relatively
small size of the series adversely affected the result. The stroke recurrence
rate was 2.04%, which was significantly low when compared to the natural history of the patients with atherosclerotic carotid artery disease which can be as high as 26.5%.[39],[40]
References
| 1. | Dyken M. Stroke risk factors. In : Norris JW, Hachinski VC, editors. Prevention of stroke. Springer-Verlag: New York, NY; 1991. p. 83-102. Back to cited text no. 1 |
| 2. | O'Leary DH, Polak JF, Kronmal RA, Kittner SJ, Bond MG, Wolfson SK, et al. Distribution and correlates of sonographically detected carotid artery disease in the Cardiovascular Health Study. Stroke 1992;23:1752-60. Back to cited text no. 2 |
| 3. | Zarins CK. Carotid endarterectomy: the gold standard. J Endovasc Surg 1996;3:10-5. Back to cited text no. 3 |
| 4. | North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. New Engl J Med 1991;325:445-53. Back to cited text no. 4 |
| 5. | Executive Committee for the Asymptomatic Carotid Atherosclerotic Study. Endarterectomy for asymptomatic carotid artery stenosis. JAMA 1995;273:1421-8. Back to cited text no. 5 |
| 6. | Thιron JG, Payelle GG, Coskun O, Huet HF, Guimaraens L. Carotid artery stenosis: treatment with protected balloon angioplasty and stent placement. Radiology 1996;201:627-36. Back to cited text no. 6 |
| 7. | Wholey MH, Wholey M, Bergeron P, Diethrich EB, Henry M, Laborde JC, et al. Current global status of carotid artery stent placement. Cath Cardiovasc Diagn 1998;44:1-6. Back to cited text no. 7 |
| 8. | Vitek JJ, Iyer SS, Roubin GS. Carotid stenting in 350 vessels: problems faced and solved. J Invasive Cardiol 1998;10:311-4. Back to cited text no. 8 |
| 9. | Yadav JS, Roubin GS, Iyer S, Vitek J, King P, Jordan WD, et al. Elective stenting of the extracranial carotid arteries. Circulation 1997;95:376-81. Back to cited text no. 9 |
| 10. | Coward LJ, Featherstone RL, Brown MM. Safety and efficacy of endovascular treatment of carotid artery stenosis compared with carotid endarterectomy: a Cochrane systematic review of the randomized evidence. Stroke 2005;36:905-11. Back to cited text no. 10 |
| 11. | Qureshi A, Kirmani JF, Divani AA, Hobson RW. Carotid Angioplasty with or without Stent Placement versus Carotid Endarterectomy for Treatment of Carotid Stenosis: A Meta-analysis. Neurosurgery 2005;56:1171-81. Back to cited text no. 11 |
| 12. | Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. New Engl J Med 1998;339:1415-25. Back to cited text no. 12 |
| 13. | Kerber CW, Hornwell LD, Loeden OL. Catheter dilatation of proximal carotid stenosis during distal bifurcation endarterectomy. AJNR Am J Neuroradiol 1980;1:348-9. Back to cited text no. 13 |
| 14. | Kachel R. Results of balloon angioplasty in the carotid arteries. J Endovasc Surg 1996;3:22-30. Back to cited text no. 14 |
| 15. | McCleary AJ, Nelson M, Dearden NM, Calvey TA, Gough MJ. Cerebral haemodynamics and embolization during carotid angioplasty in high-risk patients. Br J Surg 1998;85:771-4. Back to cited text no. 15 |
| 16. | Wholey MH, Wholey MH, Eles G. Clinical experience in cervical carotid artery stent placement. Carotid Neurovasc Intervent 1998;1:2-9. Back to cited text no. 16 |
| 17. | Serruys PW, van Hout B, Bonnier H, Legrand V, Garcia E, Macaya C, et al. Randomised comparison of implantation of heparin-coated stents with balloon angioplasty in selected patients with coronary artery disease (Benestent II). Lancet 1998;352:673-81. Back to cited text no. 17 |
| 18. | Kastrup A, Groschel K, Schulz JB, Nagele T, Ernemann U. Clinical predictors of transient ischemic attack, stroke, or death within 30 days of carotid angioplasty and stenting. Stroke 2005;36:787-91. Back to cited text no. 18 |
| 19. | Piamsomboon C, Roubin GS, Liu MW, Iyer SS, Mathur A, Dean LS, et al. Relationship between oversizing of self-expanding stents and late loss index in carotid stenting. Cathet Cardiovasc Diagn 1998;45:139-43. Back to cited text no. 19 |
| 20. | Watkinson AF. Metallic stents: individual designs and characteristics. In : Adam A, Mueller P, Dondelinger R, editors. Textbook of metallic stents. Isis Medical Media: San Francisco, Calif; 1997. p. 207-33. Back to cited text no. 20 |
| 21. | Teirstein PS, Massullo V, Jani S, Popma JJ, Mintz GS, Russo RJ, et al. Catheter-based radiotherapy to inhibit restenosis after coronary stenting. N Engl J Med 1997; 336:1697-703. Back to cited text no. 21 |
| 22. | Wholey MH. Randomizing carotid endarterectomy to carotid stenting? (editorial). J Endovasc Surg 1999;6:127-30. Back to cited text no. 22 |
| 23. | Theron J, Courtheoux P, Alachkar F, Bouvard G, Maiza D. New triple coaxial catheter system for carotid angioplasty with cerebral protection. AJNR Am J Neuroradiol 1990;11:869-74. Back to cited text no. 23 |
| 24. | Roubin GS, Iyer SS, Vitek JJ. Carotid embolic filter devices: the latest advance in carotid stenting (abstr). J Endovasc Surg 1999;6:110. Back to cited text no. 24 |
| 25. | Jordan WD, Voellinger DC, Doblar DD, Plyushcheva NP, Fisher WS, McDowell HA. Microemboli detected by transcranial Doppler monitoring in patients during carotid angioplasty versus carotid endarterectomy. Cardiovasc Surg 1999;7:33-8. Back to cited text no. 25 |
| 26. | Brown MM. Balloon angioplasty for extracranial carotid disease. Advances in Vascular Surgery Vol 4. Mosby Year Book: St. Louis; 1996. p. 53-69. Back to cited text no. 26 |
| 27. | Yadav JS, Wholey MH, Kuntz RE, Fayad P, Katzen BT, Mishkel GJ, et al. Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med 2004;35:1493-501. Back to cited text no. 27 |
| 28. | Pomposelli FB, Lamparello PJ, Riles TS, Craighead CC, Giangola G. Imparato AM. Intracranial hemorrhage after carotid endarterectomy. J Vasc Surg 1988;7:248-55. Back to cited text no. 28 |
| 29. | McCabe D, Brown M, Clifton A. Fatal cerebral reperfusion hemorrhage after carotid stenting. Stroke 1999;30:2483-6. Back to cited text no. 29 |
| 30. | Morrish W, Grahovac S, Douen A, Cheung G, Hu W, Farb R, et al. Intracranial Hemorrhage after Stenting and Angioplasty of Extracranial Carotid Stenosis. Am J Neuroradiol 2000;21:1911-6. Back to cited text no. 30 |
| 31. | Meyers PM, Higashida RT, Phatouros CC, Malek AM, Lempert TE, Dowd CF, et al. Cerebral hyperperfusion syndrome after percutaneous transluminal stenting of the craniocervical arteries. Neurosurgery 2000;47:335-43. Back to cited text no. 31 |
| 32. | Kaku Y, Yoshimura S, Kokuzawa J. Factors Predictive of Cerebral Hyperperfusion after Carotid Angioplasty and Stent Placement. Am J Neuroradiol 2004;25:1403-8. Back to cited text no. 32 |
| 33. | Coutts SB, Hill MD, Hu WY. Hyperperfusion syndrome: toward a stricter definition. Neurosurgery 2003;53:1053-8. Back to cited text no. 33 |
| 34. | Hosoda K, Fujita S, Kawaguchi T, Shose Y, Shibata Y, Tamaki N. Influence of degree of carotid artery stenosis and collateral pathways and effect of carotid endarterectomy on cerebral vasoreactivity. Neurosurgery 1998;42:988-95. Back to cited text no. 34 |
| 35. | Nicosia A, Leotta E, Moshiri S, Galassi AR, Barbagallo R, Santonocito D, et al. Carotid artery stenting in the presence of contralateral carotid occlusion: mind the hyperperfusion syndrome! Ital Heart J 2004;5:152-6. Back to cited text no. 35 |
| 36. | Abou-Chebl A, Yadav JS, Reginelli JP, Bajzer C, Bhatt D, Krieger DW. Intracranial hemorrhage and hyperperfusion syndrome following carotid artery stenting: risk factors, prevention and treatment. J Am Coll Cardiol 2004;43:1596-601. Back to cited text no. 36 |
| 37. | Henry M, Gopalakrishnan L, Rajagopal S, Rath PC, Henry I, Hugel M. Bilateral carotid angioplasty and stenting. Catheter Cardiovasc Interv 2005;64:275-82. Back to cited text no. 37 |
| 38. | Kihara EN, Andrioli MS, Zukerman E, Peres MF, Porto Junior PP, Monzillo PH, et al. Endovascular treatment of carotid artery stenosis: retrospective study of 79 patients treated with stenting and angioplasty with and without cerebral protection devices. Arq Neuropsiquiatr 2004;62:1012-5. Back to cited text no. 38 |
| 39. | Wilterdink JL, Easton JD. Vascular event rates in patients with atherosclerotic cerebrovascular disease. Arch Neurol 1992;49:857-63. Back to cited text no. 39 |
| 40. | Matzsch T, Bergqvist D, Lindh M, Maly P, Takolander R. Natural history of patients with unoperated atherosclerotic carotid artery disease - result from a retrospective study. Eur J Vasc Surg 1993;7:166-70. Back to cited text no. 40 |
Copyright 2006 - Neurology India
The following images related to this document are available:
Photo images
[ni06018t1.jpg]
[ni06018f4.jpg]
[ni06018f3.jpg]
[ni06018f2.jpg]
[ni06018t2.jpg]
[ni06018f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}