 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
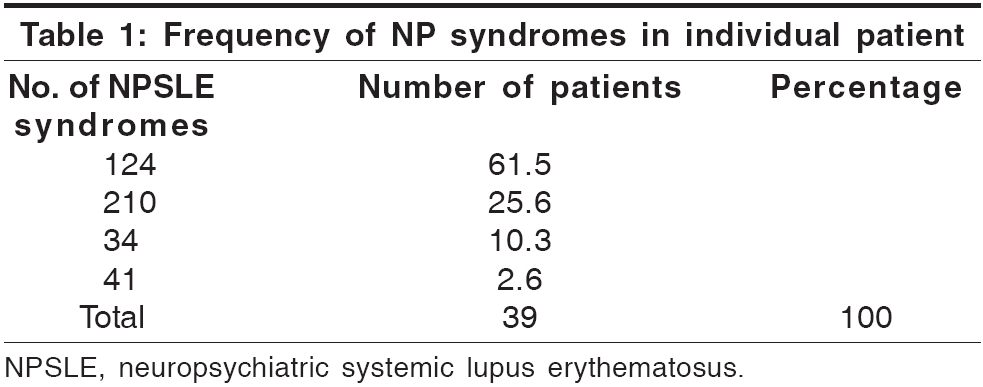
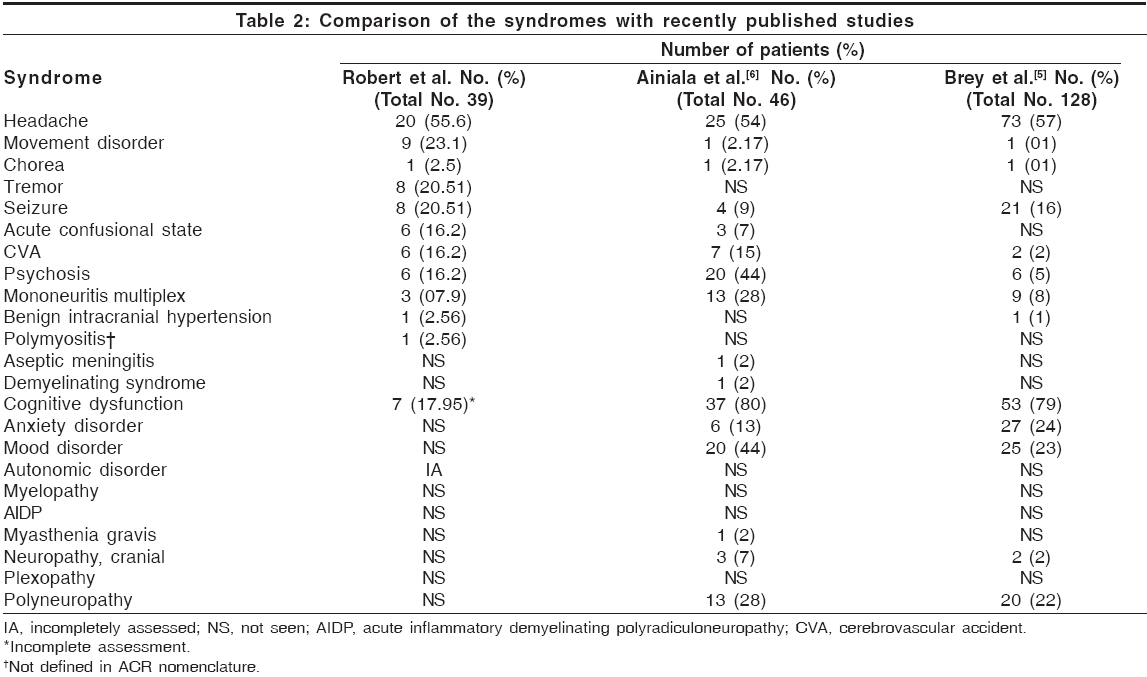
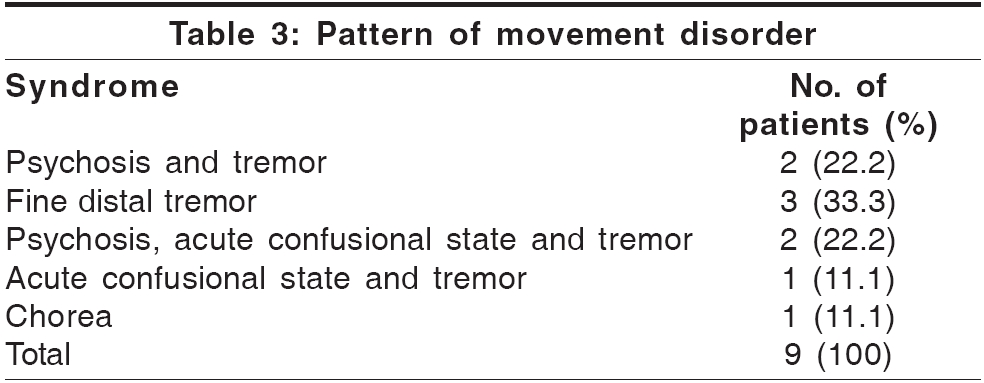
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 75-77 Brief Report Neuropsychiatric manifestations systemic lupus erythematosus: A study from South India Robert M, Sunitha R, Thulaseedharan NK Departments of Neurology, Medical College Hospital, Trivandrum, Kerala Code Number: ni06020 Abstract Context: Neuropsychiatric systemic lupus erythematosus (NPSLE) has varied manifestations.Aims: To study the pattern of neuropsychiatric (NP) involvement in systemic lupus erythematosus (SLE). Settings and Design: Hospital based cross sectional and retrospective study. Patients and Methods: Patients admitted with a diagnosis of SLE, during a period of 16 months, were evaluated and any NP syndrome present classified as per the American College of Rheumatology (ACR) nomenclature. Statistical analysis: SPSS software Version 10 was used for descriptive analysis and correlative study. Results: Out of 50 patients with SLE, all the patients with NPSLE [39 (78%)] were females, mean age 25.66 years (range: 11-44). The commonest manifestation was headache [20 (55.6%)]. Seizures were seen in 8 (20.51%) and psychosis in 6 (16.2%). Fine distal tremor was seen in 8 (20.51%) of patients. Conclusions: Headache is a frequent NP syndrome. Fine distal tremor is a syndrome not included in ACR classification but seen is 20% of our patients with NPSLE. Keywords: Neurolupus, neuropsychiatric syndromes, neuropsychiatric systemic lupus erythematosus, systemic lupus erythematosus. The prevalence of neuropsychiatric systemic lupus erythematosus (NPSLE) in systemic lupus erythematosus (SLE) ranges widely between 14 and 75%, reflecting variable diagnostic criteria and differences in selection of patients for study. The American College of Rheumatology (ACR) has recently developed a standardized nomenclature system, which provides case definitions for neuropsychiatric (NP) syndromes seen in SLE. Regional variability has been described, blacks and hispanics being affected much more frequently than whites. To the best of our knowledge this is the largest series of patients with NPSLE reported from this part of the country.[1],[2],[3] Materials and Methods The study was a cross sectional and retrospective, descriptive study. Patients admitted to various adult wards in a tertiary referral center in South India during a period of 16 months from June 2003 to September 2004, satisfying American Rheumatologic Association criteria for SLE were included. Neuropsychiatric syndromes were classified as defined by the ACR. Medical reports were analyzed and NP syndromes diagnosed earlier were also included. Even though the ACR classification lists out the investigations required to make the diagnosis of each NPSLE syndrome, only those investigations, which were of prime importance to make a diagnosis were done. Statistical analysis Results Fifty patients with SLE were identified, 46 females and 4 males. Mean age was 24.94 years (SD: 7.9; range: 11-45). Indication for admission was neurological in 16 (32%), renal in 15 (30%) and others (arthritis, fever, etc.) in 19 (38%). Of the 50 patients 39 (78%) had at least one NP syndrome. All were females of mean age 25.66 years (range: 11-45). Mean duration of systemic illness was 36.11 months (SD: 32.12; range: 1-120) and neurological illness 29.3 months (range: 0.25-108; SD: 32.03). Out of 39 patients with NPSLE 26 (67%) had lupus nephritis also. Exact duration of both systemic and neurological illness was known only in 28 patients. In 15 (53.57%) patients NPSLE followed the onset of other systemic illness, the reverse in 7 (25%) and simultaneous onset in 6 (21.43%). The mean ESR value was 76.66 (SD 43.80) when the mean of the non-NPSLE group was 88 (SD 49.56). The mean urea value was 45.44 mg% (SD 9.24) and creatinine 1.27 (SD 0.25). As treatments, 89.74% of the patients were on steroids and 56.41% had received parenteral steroid. A total of 60 syndromes were diagnosed in 39 patients. Detailed cognitive assessment and autonomic function could not be done in many of the sick patients because of technical reasons and was hence not included in the final analysis. However the mean MMSE score was 26.89 (SD 2.56) and cognitive dysfunction as assessed by clinical examination alone was seen in 7 (17.95%) patients. Twenty-four (61.5%) patients had only one syndrome while one patient had 4 [Table - 1]. The commonest syndrome was headache [20 (55.6%) patients]. Of this 10 (50%) had vascular and 10 (50%) tension headache. Headache was the only neurological manifestation in 14 (35.9%) patients. The least common syndromes were benign intracranial hypertension and polymyositis (one patient each). Aseptic meningitis, demyelinating syndrome, anxiety disorder, mood disorder, myelopathy, acute inflammatory demyelinating polyradiculoneuropathy, myasthenia gravis, cranial neuropathy, plexopathy, and polyneuropathy were the syndromes not seen in any patients. On Pearson correlation analysis, significant correlation was found between cerebrovascular accident (CVA) and acute confusional state ( P = 0.01). No correlation was found with age. The syndromes were compared with those described in recently published series [Table - 2].[4],[5],[6] Of the 19 patients imaged 15 had CT scans, two had MRI scans and one patient had both. Imaging was normal in 7 (36.84%) and abnormal in 12 (63.16%). Infarcts were seen in six patients and generalized atrophy in four. In two patients the abnormality could not be properly characterized. An abnormal imaging had a significant correlation with CVA ( P < 0.0001) and a normal imaging has significant correlation with psychosis ( P < 0.0001). Of the nine patients with movement disorder, eight had tremor. The tremor was fine and distal more during posture and less during rest and action. In three patients this was the only NP manifestation. The rest of the patients were having either psychosis or acute confusional state along with the tremor [Table - 3]. Plain CT scan was available in four patients and showed generalized atrophy in two and normal study in two. None of the patients had clinical evidence of thyrotoxicosis or Parkinsonism. A thyroid function test could be done in one patient, which was normal. One of the patient′s mothers also had similar tremor. All the patients were on steroids, and those with psychosis were on neuroleptics and hence drug induced tremor could not be ruled out. In none of the patients did the tremor improve with further immunomodulation. Significant correlation of tremor was seen with headache ( P =0.013). Discussion The study describes NP syndromes significant enough to warrant hospitalization as well NPSLE syndromes occurring in SLE patients who are significantly morbid from other systemic illness. These patients are candidates for aggressive management and are likely to be more sensitive to measures of treatment response. The available hospital based studies, had not adopted the ACR nomenclature system and hence could not be used for comparison. Hence the findings were compared with two recently published community based studies. The prevalence of headache as well as chorea was comparable in all the three studies. Prevalence of seizure and stroke was similar to one of the studies each. Cognitive involvement could not be studied in detail in these patients because of technical reasons. Cognitive assessment requires neuropsychological assessment. This is time consuming (1-4 h as recommended by ACR) and needs wholehearted co-operation, which was not readily forthcoming in this cohort of sick patients.[6] Presence of aphasia, psychosis etc also interfered with assessment. Earlier series, which were hospital based did not give much importance to cognitive impairment.[7],[8] An interesting and new finding was the tremor disorder seen in 8 (20.51%) of our patients. This syndrome has not been defined in the ACR nomenclature and rare in literature.[9],[10] All the patients had bilateral distal fine tremor, prominent during posture and action. This type of tremor can occur in essential tremor syndrome or as part of enhanced physiologic tremor, due to drugs or fatigue. Drug induced tremor could not be ruled out in any patients. It is likely that some or all of these factors were responsible for tremor in our patients either causally or as a contributory factor. The available imaging did not show any focal abnormalities. It is likely that this sign was not detected in many patients as index of suspicion was low and it did not often produce any symptoms. Small sample size, lack of exhaustive investigations and cognitive assessment significantly limits the findings of this study. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06020t2.jpg] [ni06020t1.jpg] [ni06020t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}