 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
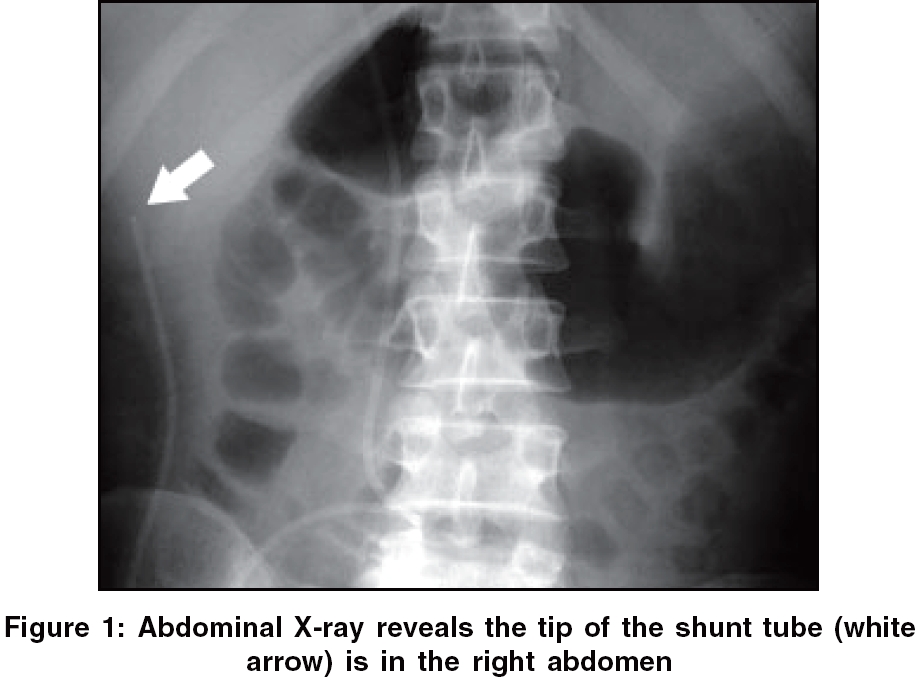
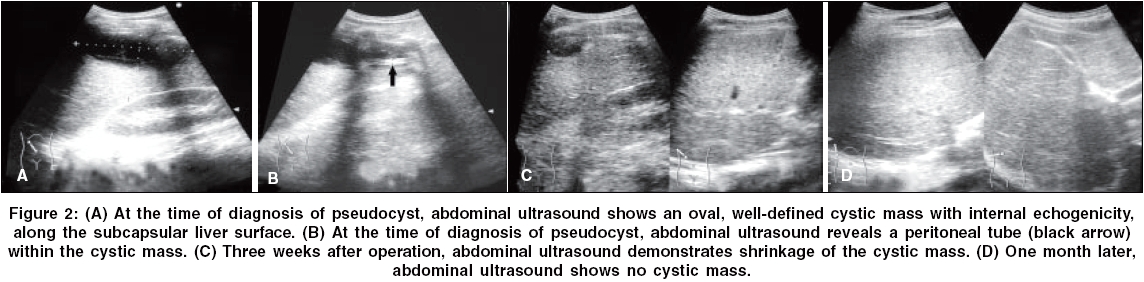
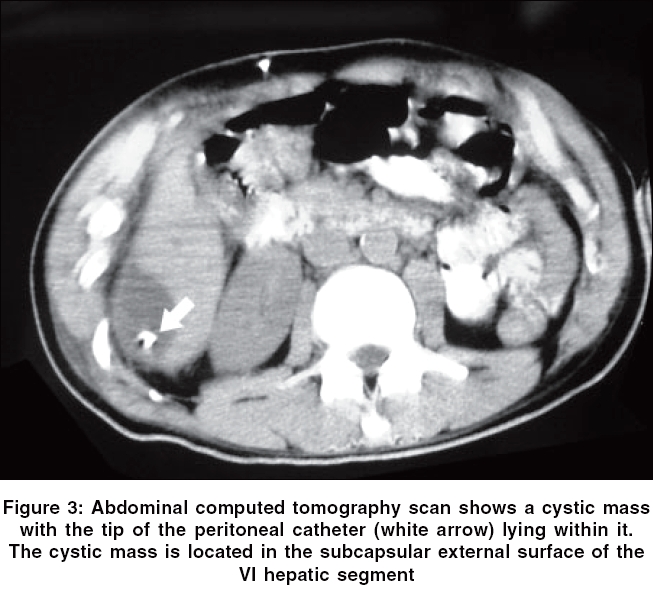
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 86-88 Case Report Hepatic cerebrospinal fluid pseudocyst: A case report and review of the literature Hsieh CT, Pai CC, Tsai TH, Chiang YH, Su YH Departments of Neurological Surgery, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China Code Number: ni06024 Abstract An abdominal pseudocyst is a rare, but important complication in patients with a ventriculo-peritoneal (VP) shunt insertion. Several predisposing factors for this complication have been suggested, including infection, obstruction or dislodgement, but the pathophysiology is still unknown. However, the abdominal inflammatory process is accepted widely as a hypothesis for the formation of an abdominal pseudocyst. In this study, we report the case of a 21-year-old male that presented with a high-grade fever, poor appetite, shortness of breath and unconsciousness 1 week after receiving a VP shunt insertion for obstructive hydrocephalus. Ultrasonography and computed tomographic scans of the abdomen revealed a well-defined large hepatic cyst surrounding the peritoneal tube of the VP shunt. A hepatic cerebrospinal fluid (CSF) cyst was diagnosed and Staphylococcus epidermis was cultured via CSF. After externalization of the VP shunt and adequate antibiotic treatment, the hepatic cyst was resolved. There was no recurrence observed in the regular follow up.Keywords: Abdominal pseudocyst, hydrocephalus, ventriculoperitoneal shunt The formation of an abdominal cerebrospinal fluid (CSF) pseudocyst, which was first described by Harsh in 1954,[1] is rarely reported in patients with a ventriculo-peritoneal (VP) shunt.[2] Unspecific clinical presentations may cause diagnostic and therapeutic difficulties, therefore, physicians should be aware of this complication, especially in unconscious patients. Here, we report a case of an unconscious patient that presented with a hepatic CSF pseudocyst after VP shunt insertion. Case Report A 39-year-old male, who has no history of malignancy, pancreatic or liver disease, sustained a head injury during a motor vehicle crash. On arrival, the Gasgow Coma Scale score was E3M4Vt. Laboratory examinations revealed an elevation in aspartate aminotransferase (AST) levels (77 U/l) and emergent ultrasonography of abdomen demonstrated no remarkable findings. A nonenhanced computed tomographic (CT) scan of the head showed a fracture of the skull, intracerebral hemorrhage and hydrocephalus. A VP shunt insertion for hydrocephalus was performed at 1 month after admission. However, at 1 week after the VP shunt insertion, he developed a high-grade fever and poor appetite, followed by shortness of breath and unconsciousness. Physical examinations showed no significant findings except a high-grade body temperature (38.7°C). No malfunction of VP shunt was also noted. Laboratory examinations revealed elevations in the white blood cell count (16900/μl), C-reactive protein levels (14.32 mg/dl), erythrocyte sedimentation rate (90 mm/h), AST levels (50 U/l) and alanine aminotransferase levels (54 U/l). CSF studies showed no abnormal findings. Follow-up brain CT revealed no enlargement of the ventricular size. A plain X-ray of the abdomen showed that the tip of the VP shunt was located in the right upper quadrant [Figure - 1]. An oval, well defined cystic mass with internal echogenicity, along the subcapsular liver surface was found by ultrasonography of abdomen [Figure - 2]A and the peritoneal tip of the VP shunt seemed to be located within the cyst [Figure - 2]B. Our initial diagnostic impression was an abdominal abscess. However, a large, nonenhanced cystic mass with homogenous low attenuation in the subcapsular external surface of the VI hepatic segment measuring approximately 6 x 4 x 10 cm in size was noted at CT scan of abdomen [Figure - 3]. A hepatic CSF pseudocyst secondary to the migration of the VP shunt was highly suspected. Therefore, he underwent distal externalization of the VP shunt. CSF culture demonstrated a Staphylococcus epidermis infection and adequate antibiotic treatment was administrated. The previous symptoms improved later. At 3 weeks after this operation, ultrasonography of the abdomen showed shrinkage of the cyst [Figure - 2]C. After the infection was well controlled, the VP shunt was reinserted. One month later, the patient was discharged with complete resolution of the cyst [Figure - 2]D.Discussion An abdominal pseudocyst, also called a peritoneal cyst, omental cyst, or intraperitoneal pseudocyst, is an uncommon, but well-known complication of VP shunts.[3] It consists of a collection of CSF in the peritoneal cavity at the catheter tip and is surrounded by a wall composed of fibrous tissue without an epithelial lining.[2] The incidence varies from 0.33 to 6.8% and a hepatic CSF pseudocyst has rarely been reported in the English literature.[2] The etiology for pseudocyst formation is still unknown. Currently, inflammatory process, either sterile or infectious, is generally regarded as the main causative factor.[2],[3],[4],[5] The infection rate has been reported to be from 17 to 80% and S. epidermis and Staphylococcus aureus are the most commonly cultured micro-organisms.[2],[3],[5] Other predisposing factors have been postulated such as peritonitis, prior surgical peritoneal adhesion, distal shunt migration, multiple shunt revisions, malabsorption of CSF and allergic reaction.[4],[5],[6] The most frequent symptoms and signs of abdominal pseudocysts are abdominal pain (63%), abdominal distension (37%), abdominal tenderness (31%) and abdominal mass (29%).[7] In a review of fourteen cases, children mainly complained of symptoms of elevated intracranial pressure, such as headache and nausea and adults predominantly suffered local abdominal signs.[4] The time between last VP shunt operation and development of abdominal pseudocysts has been reported from 3 weeks to 10 years.[8] The suspicion of abdominal pseudocyst is often made at the time of physical examination and on the basis of conventional radiology. Ultrasonography is the method of choice because it is fast and reliable.[2] Imaging findings may show a large fluid-filled collection containing debris and the VP shunt catheter close to the walls.[9] Besides, the double echo of the catheter walls may produce the so-called railroad sign within the pseudocyst.[4] Furthermore, a CT scan of the abdomen provides a more accurate diagnosis, especially when abdominal pseudocyst is not defined by ultrasonography.[9],[8] In differential diagnoses of abdominal cystic mass, one has to consider as metastastic disease from the brain through VP shunt, cyst of mesentery or omentum, small bowel duplication cyst, seroma, lymphocele, cystic teratoma, cystic spindle cell tumor, cystic lymphangioma, pancreatic pseudocyst, biloma, urinoma and abdominal abscess.[4],[8] Abdominal abscess, biloma, urinoma and pancreatic pseudocyst most frequently mimic a pseudocyst in a post-traumatic patient. However, the accurate diagnosis of abnormal pseudocysts is difficult based on laboratory examination or images findings alone. Fine-needle aspiration may help us make the diagnosis more exactly.[8] Currently, the treatment protocol for abdominal pseudocyst is controversial. Surgery, such as a wide excision of the cystic walls, CT-guided or sono-guided aspiration of the pseudocysts and shunt externalization or revision, has been report to be curative.[3],[5],[9],[10] If infection is suspected, many authors suggest that it is essential to place a temporary extraventricular device and to administer adequate antibiotic treatment.[3],[5],[6],[9] According to this procedure, Mobley et al. applied a treatment algorithm treated abdominal pseudocysts according to the suspicion of shunt infection.[2] In our case, the formation of the hepatic pseudocyst may be caused by focal injury of the liver surface through migration of the peritoneal tip of the shunt. Besides, some sort of liver laceration at the time of initial injury may also allow a point of entry for shunt tip. In conclusion, an abdominal pseudocyst should be included in the differential diagnosis of an acute abdominal compliant and can be easily and quickly diagnosed by ultrasonography. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06024f2.jpg] [ni06024f3.jpg] [ni06024f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}