 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
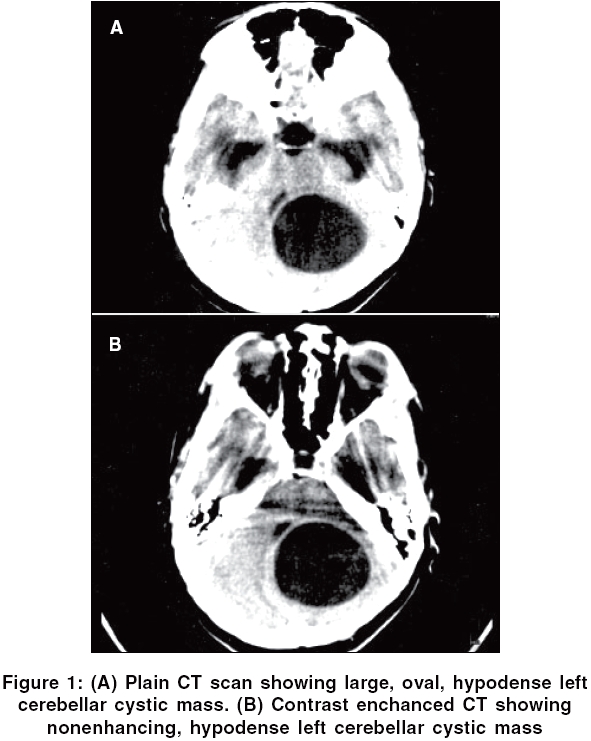
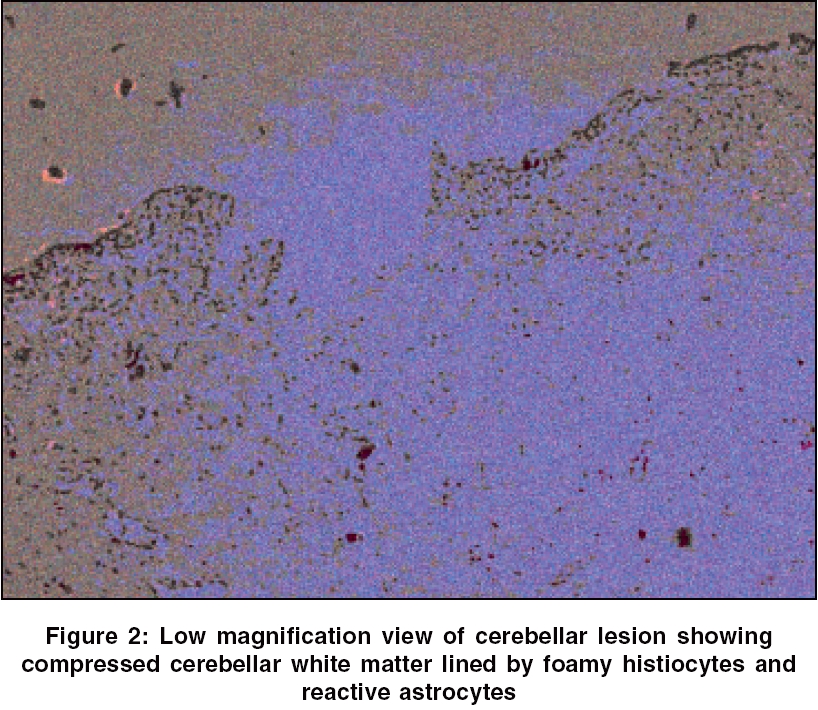
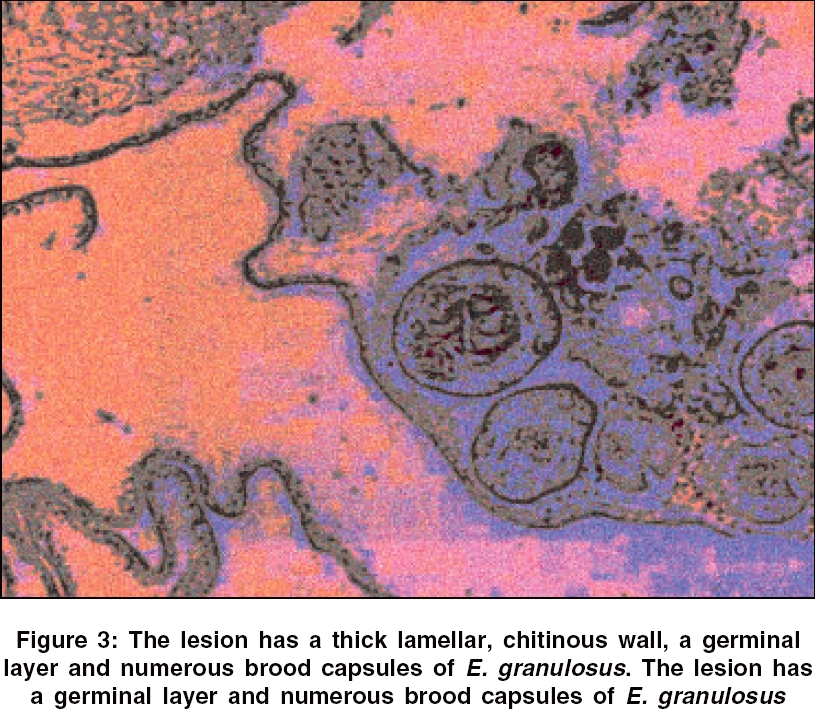
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 100-101 Neuropathological Discussion 13-year-old boy with cerebellar cystic mass Yasha TC, Shibu P, Srikanth SG, Shankar SK Departments of Neuropathology, NIMHANS, Bangalore Code Number: ni06029 A 13-year-old boy presented to the neurosurgical services with complaints of bifrontal headache for 1 year and progressive deterioration of vision in both eyes. The headache had worsened for the past 1 month, associated with vomiting at the height of headache. Fifteen days prior to admission to the hospital his visual acuity worsened to an extent just to perceive light. General systemic examination was normal. The neurological evaluation revealed visual acuity of only perception of light, bilateral secondary optic atrophy, right sixth cranial nerve paresis, and left cerebellar signs. On cranial CT scanning an oval, hypodense [Figure - 1]A left cerebellar cystic mass was noted, nonenhancing with contrast [Figure - 1]B. Fourth ventricle was compressed with resultant hydrocephalus. With a clinical diagnosis of cystic cerebellar tumor, the cyst was excised by suboccipital craniectomy. The cyst ruptured during the surgery and was found to be lined by thin white membrane and filled with xanthochromic fluid. Pathological examination Diagnosis: Hydatid cyst in cerebellum Discussion E. granulosus (Hydatidosis) infestation is a zoonotic disease, humans getting infected accidentally as intermediate hosts. The disease is transmitted usually by food-borne contamination by eggs passed in faeces of definitive host, mainly dogs. E. granulosus infestation results in liver cysts in nearly half the cases and brain involvement is less than 5%. The symptomatology, depends crucially on the location of the cyst in the brain.[1] The infestation may be primary often presenting as solitary parenchymal cyst. Secondary involvement is due to cyst rupture or hydatid fluid dissemination from a distant organ, by haematogenous route. CNS echinococcosis is rare in infants and more common in children up to 15 year of age than in adults. The signs and symptoms include raised intracranial pressure, headache, vomiting, papilloedema, hemiparesis and occasionally seizures.[1] The cyst lodges frequently in the cerebral hemisphere, attaining a large size. Involvement of the cerebellar hemispere and presenting radiologically as a cystic mass, is usually mistaken for cerebellar astrocytoma as in the present case. Slight or lack of ring enhancement or marginal edema on MRI should arouse suspicion of hydatidosis, especially in paediatric age patients from the tropics.[2] Recently in vivo proton magnetic resonance spectroscopy has been able to identify intracranial hydatid and other parasitic cysts from other cystic lesions.[3],[4] Rupture of the cyst during surgery may trigger anaphylaxis followed by disseminated infection.[5] At our center, a female child was operated on thrice to resect the cysts and each time a new crop appeared again. Laboratory diagnosis by ELISA, immunoblot and indirect immunofluorescence to detect the antigen and immune complexes assist in diagnosis. Negative serological tests do not rule out the disease. Live cyst elicits negligible host reaction and surgical specimens rarely include brain tissue. The cyst undergoing degeneration, elicits epitheloid and giant cell reaction, finally leaving behind amorphous necrotic debris surrounded by dense gliosis. Following infestation by E. parasite , the host develops an immunological response protective against reinfection, but not effective against the lodged parasite. Evasion of the host immune attack against the parasite is mediated by the suppression of T-lymphocyte function and inhibiting macrophage-lymphocyte interaction.[6] Persistent production of 1L-4 as a result of chronic infection could lead to enhanced production of IgG4 antibodies, which probably act as blocking antibodies, binding with lipoprotein antigen B in hydatid cyst, thus down regulating the host response and protecting against anaphylaxixs.[7]References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06029f3.jpg] [ni06029f1.jpg] [ni06029f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}