 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
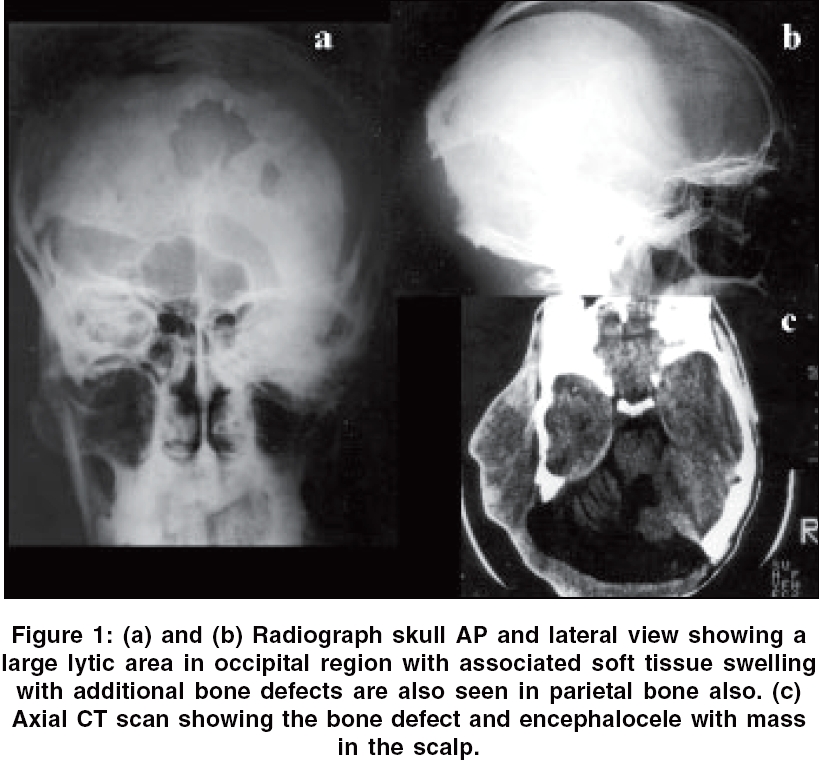
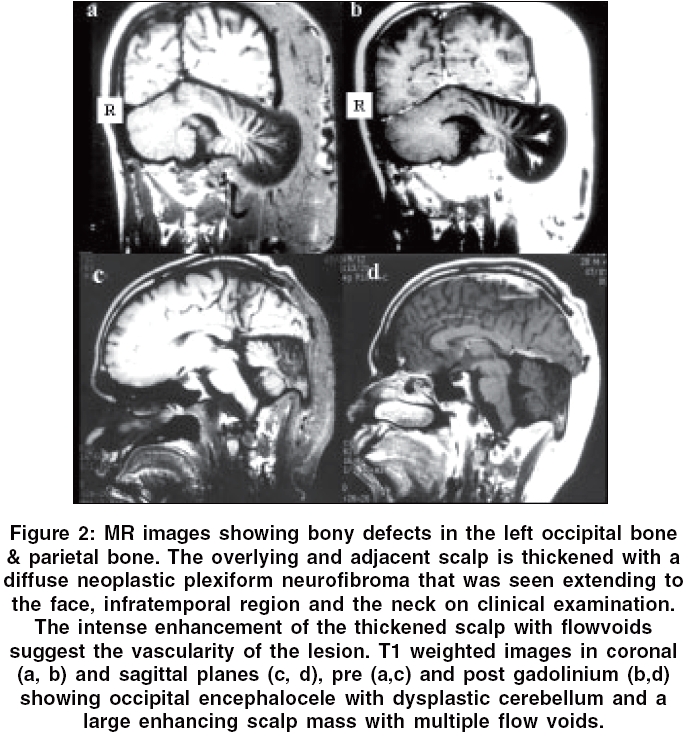
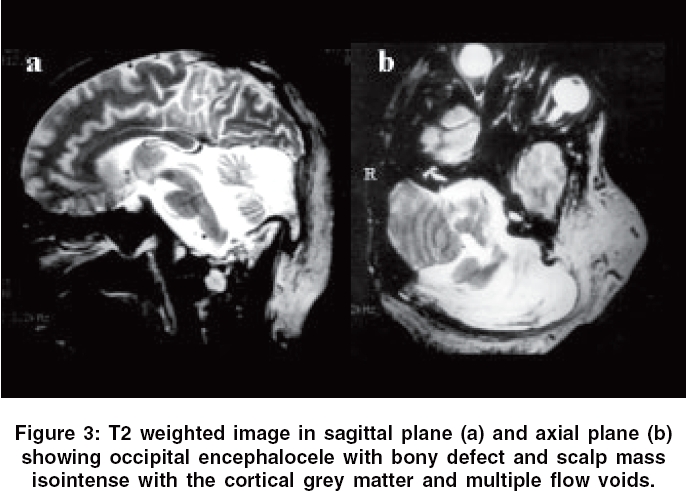
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 103-104 Letter To Editor Neurofibromatosis type I with occipital encephalocele Bodhey NK, Gupta AK Departments of Imaging Sciences and Interventional Radiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala Code Number: ni06031 Sir, Neurofibromatosis Type I is an autosomal dominant disorder associated with diverse intracranial and calvarial lesions. We present a case report of a patient with NF Type I with occipital encephalocele, an unusual association that has been described in only 1 case so far in the literature to the best of our knowledge. A 28-year-old male patient with classical cutaneous stigmata of NF - I (neurofibromas and café-au-lait spots) with plexiform neurofibroma of the scalp presented with history of gradual increase in the size of his scalp swelling over the last three months. He was subjected to a pre and postcontrast cranial MRI to know the nature of the scalp swelling, after routine skull radiographs [Figure - 1]a and b and CT [Figure - 1] c. MRI was suggestive of occipital encephalocele with plexiform neurofibroma of the scalp and neck [Figure - 2][Figure - 3]. Subsequent biopsy of the scalp lesion revealed neurofibrosarcoma on histopathologically. NF-I is the commonest of all the phakomatoses (one in 2000 to 3000 live births), is usually inherited as autosomal dominant disorder. CNS manifestations associated with NF-I are gliomas (opticochiasmatic, hypothalamic, brainstem), non-neoplastic hamartomas of white matter and basal ganglia, macrocephaly, hydrocephalus, skull and meningeal dysplasias and plexiform neurofibromatosis, neurofibromas of spinal nerves.[1] Wide variety of calvarial defects described includes those involving sphenoid,[2] frontal, parietal bones, sagittal and lambdoid suture and even the rare cranium bifidum. None of the studies have reported occipital dysplasia in NF 1 except by Renshaw et al in 2003.[3] These bony defects are because of progressive mesodermal dysplasia and rarely due to neurofibromatosis tissue in the scalp causing secondary erosion. On the contrary, in congenital cephaloceles the bone defect is in occipital bone plus the posterior arches of adjacent cervical spine or in the occipital bone alone either superior or inferior to the external occipital protuberance.[4] They can be associated with Chiari II and III malformation, Dandy Walker malformation, Cerebellar dysplasias, Diastematomyelia and Klippel-Feil syndrome. The cerebellum within those cephaloceles is usually dysplastic and gliotic.[5] Plexiform NF, hallmark of NF-I are found in 30-40% of all patients with NF-I. They usually arise along the axis of a major nerve, are unencapsulated and infiltrate producing fusiform appearance. They commonly occur along orbital division of V nerve, but other areas are not exempt often associated with sphenoidal dysplasias, they are hypervascular and enhance intensely on post contrast MR. Our patient had an occipital encephalocele with dysplastic cerebellum. However, the presence of additional parietal bony defects a finding well described in NF-I and the associated plexiform neurofibroma of the adjacent scalp suggests that the bony defect in our case could be due to the mesodermal dysplasia of NF-I. The peculiarity of this case of NF-I lies not in the presence of plexiform NF, bony dysplasia or cephalocele, findings well documented in literature, but in their unusual occipital location a site hitherto reported till now only in one case so far to the best of our knowledge. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06031f3.jpg] [ni06031f2.jpg] [ni06031f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}