 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
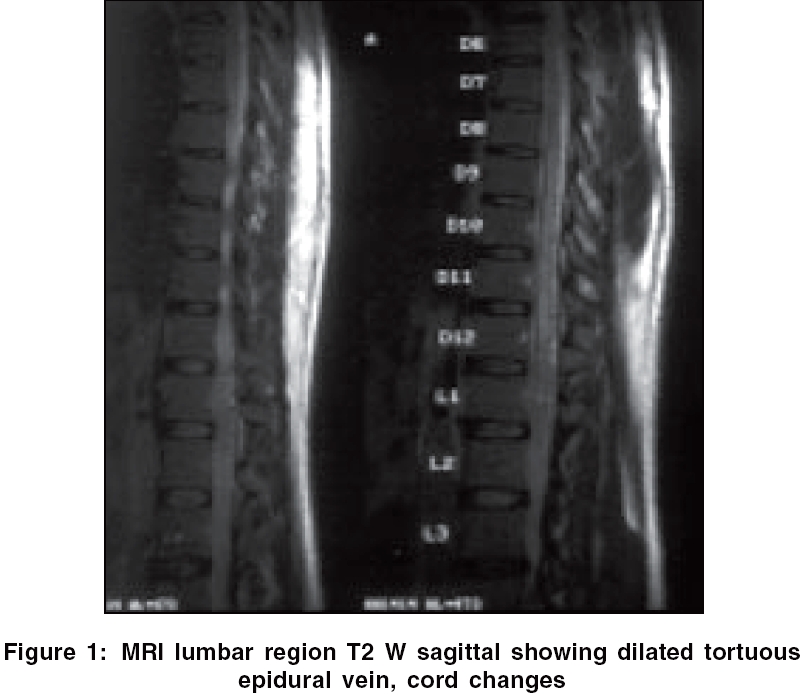
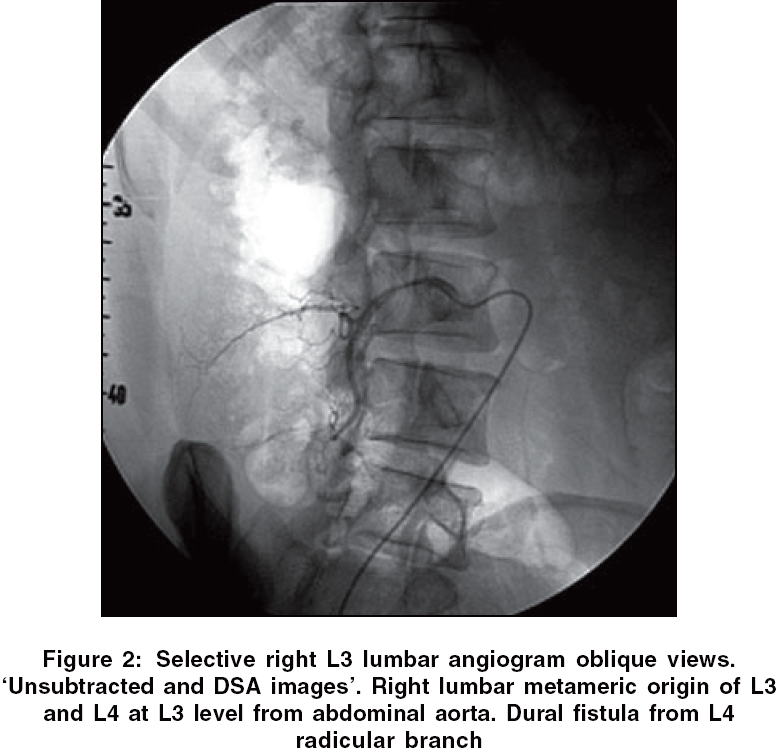
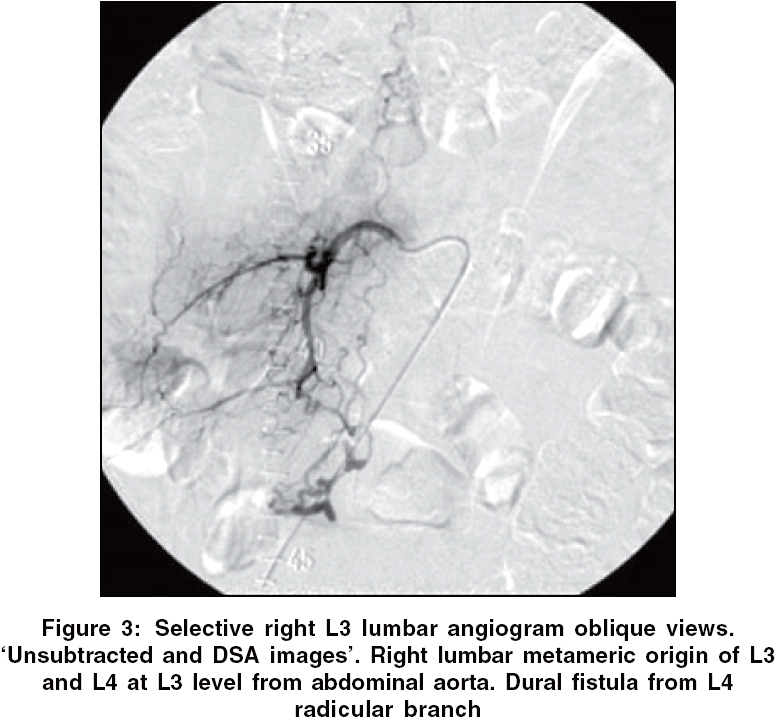
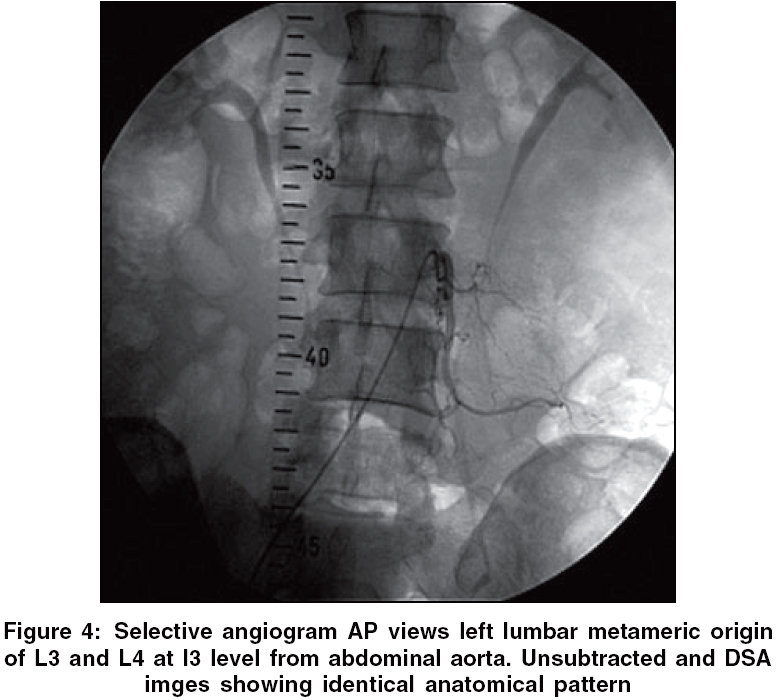
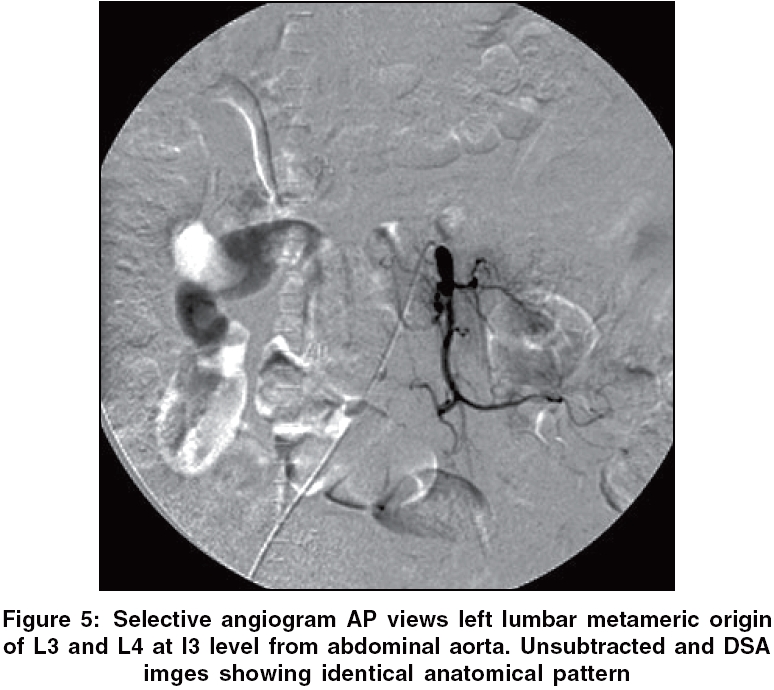
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 105-107 Letter To Editor Lumbar spinal dural arteriovenous fistula with a supply from a lumbar multimetameric arterial system Kota GopiKrishna, Shyamkumar NK, Surendrababu NRS, Rajshekhar Vedantam Departments of Radiology, Christian Medical College, Vellore Code Number: ni06033 Sir, Spinal dural arterio-venous fistulas (AVF) are abnormal arterio-venous communications on the surface of the dura. They are supplied by the branches of the vertebral, intercostals, lumbar, middle sacral or subclavian arteries and rarely by the branches of the internal iliac artery. SDAVFs represent at least 35% of all spinal vascular malformations in large series.[1] A 50-year-old male presented to the neurosurgical department with burning sensation of foot bilaterally with episodes of urinary retention and progressive weakness in right lower limb for the last one month. There was mild spasticity of both lower limbs, right more than left, with grade 5/5 power. However, the day before surgery his power in the lower limbs worsened suddenly to grade 4/5 in proximal and grade 3/5 in the distal muscle group. Deep tendon reflexes in the lower limbs were exaggerated, right more than left. The anal and cremasteric reflexes were absent. MRI of the dorso-lumbar spine [Figure - 1] was highly suggestive of a dural AVF with abnormal tortuous intradural flow voids in T2 WI seen in the thoracolumbar region. There were hyperintensities within the spinal cord at this level. Spinal angiogram [Figure - 2][Figure - 3][Figure - 4][Figure - 5] showed metameric lumbar arteries L3 and L4 with its common trunk arising at L3 level from aorta bilaterally. Fistula was demonstrated from right L4 radicular branch with tortuous draining vein seen extending upwards up to midthoracic level. No supply was noted from iliac arteries bilaterally. The day before surgery, patient developed worsening of limb paraparesis and urinary retention. The patient was surgically treated by L3-L5 laminectomy and disconnection of AV fistula. Intraoperatively on opening the dura, large arterialized vein was seen at the L4/5 level on right sde at site of exit of L4 nerve root. Temporary aneurysm clip was applied and vein changed color to blue. No change in motor evoked potential (MEP) was noted after 5 min of clipping. The vein was coagulated and cut between clips. The dural sleeve on the root was also coagulated. Patient recovered postoperatively but developed urinary retention after 2 days, which improved within 2 weeks. His motor power returned to normal in the lower limbs over a week. The vascular anatomy of vertebral spinal axis is determined during the first few weeks of development. Thirty-one somites are formed, each receiving one pair of segmental arteries form dorsal aorta. In thoracic and lumbar regions, a paired segmental arrangement persists into adulthood with minor changes in appearances attributed to differential longitudinal growth of spinal cord and vertebral column. This growth accounts for the increasing obliquity of the nerve roots and correspondingly, the radicular arteries in relation to their named intercostals and lumbar arteries. SDAVF represents an arteriovenous (AV) shunt that occurs within the dural covering of the spinal cord. Spinal arteriovenous malformations behave as shunts with the arteries communicating directly with veins rather than through the capillary bed.[2] Although MR may be very suggestive of the presence of SDAVF, spinal angiography remains the gold standard for confirming the diagnosis, localizing the level of the abnormal AV shunt, and providing sufficient information to plan and perform therapy. Angiographically the feeding vessel of SDAVFs is almost invariably a single pedicle and is not dilated; a small microfistula can be observed with a single coiled draining vein. Variations in arterial supply are well known. At lumbar level, midline common origins of the trunk supplying both sides are more frequent than longitudinal lateral bimetameric ones. The median location of the aorta favours this arrangement.[3] To prevent inadvertent compromise of the spinal cord blood supply at surgery, a complete arteriographic study is often necessary to delineate the abnormality and to define the anatomical features of the blood supply to the spinal cord in the vicinity of the dural AVF.[4] Our case has a variation in which there is longitudinal lateral bimetameric artery at L3 level, which is less common and with radicular artery from right L4 level supplying a spinal dural AVF, which is extremely rare. In conclusion, a detailed understanding of the anatomy is important for the appropriate management in such situations. Complete spinal arteriographic evaluation is very important, as there can be variations in arterial anatomy as in this case, which has provided sufficient and essential information to plan and perform therapy. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06033f2.jpg] [ni06033f5.jpg] [ni06033f3.jpg] [ni06033f4.jpg] [ni06033f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}