 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
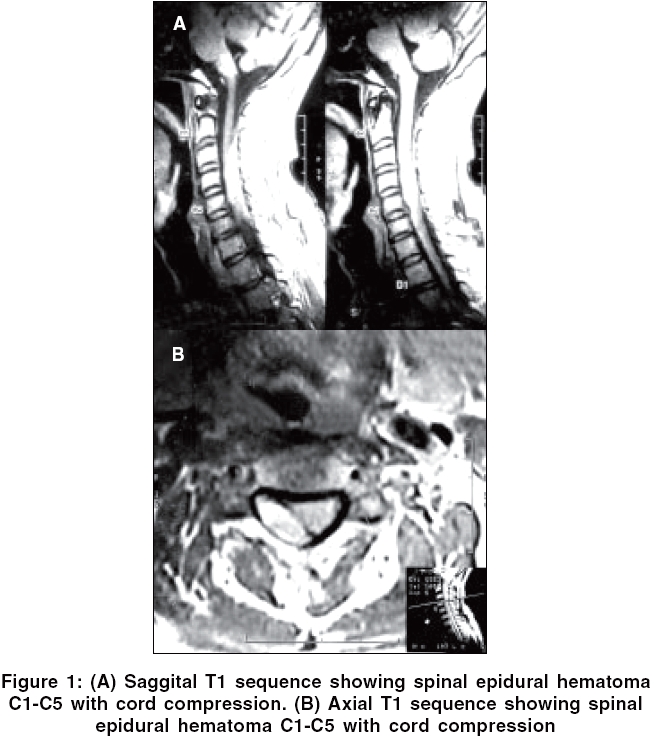
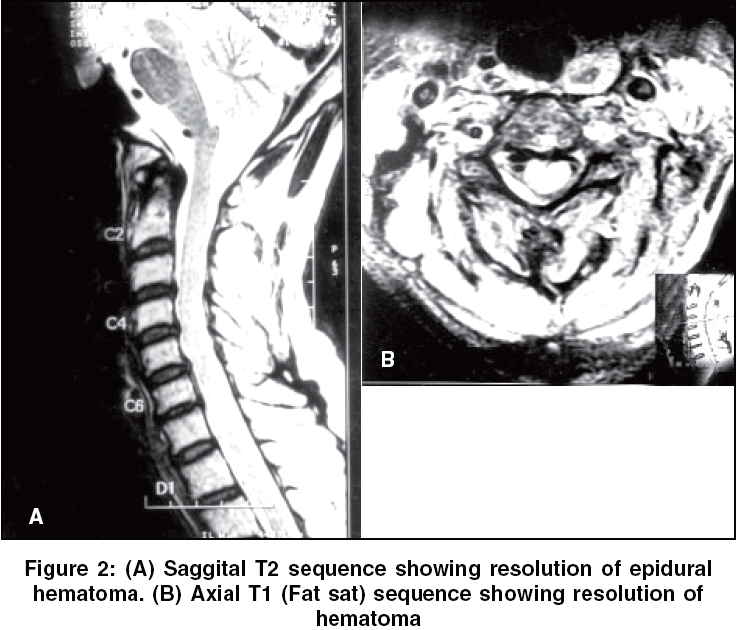
Neurology India, Vol. 54, No. 1, January-March, 2006, pp. 107-108 Letter To Editor Cervical spinal epidural hematoma with acute Brown-Séquard presentation Neetu R, Chandra MS, Rashmi M Departments of Neurology, Rungta Hospital, D-694, Malviya Nagar, Jaipur - 302 017 Code Number: ni06034 Sir, Spinal epidural hematoma (SEH) is rare. The SEH may be primary or secondary to other underlying causes such as trauma, anticoagulant therapy, vascular anomalies, blood dyscrasias, and epidural anesthesia.[1] A 55 years male complaints of severe neck pain radiating to inter-scapular region of acute onset without any precipitating factor. He underwent chiropractic manipulation for relief of neck pain and then received low-molecular weight heparin fraxiparin (nadroparin) 0.6 mg twice daily with aspirin (150 mg) and clopidogrel (75 mg) in the mistaken belief that the pain was cardiac in origin. In next 48 h patient developed right sided weakness with paraesthesias in both upper limbs and bladder disturbances in form of frequency and urgency. Neurological examination revealed normal higher mental functions, cranial nerves (11th not tested due to severe pain), and ocular fundi. He had a grade (MRC) 1/5 power in right shoulder, 3/5 in elbow, and 4/5 at wrist. Right hip was 4/5 and distally power was 5/5. Left shoulder power was 4/5. All other joints on left side had normal power. Right biceps jerk (BJ), triceps jerk (TJ), and supinator jerks (SJ) were not elicitable. Left BJ, TJ, and SJ were 2+. Bilateral knee and ankle jerks were brisk with extensor planters. Sensory examination revealed diminished pinprick on left side without any definitive level. Proprioceptive sensations were normal. Neck movements were restricted and tender. A clinical diagnosis of compressive cervical myelopathy was made in view of acute Brown-Séquard presentation suggesting spinal hemi paresis. It was confirmed by MR imaging of the cervical spine, which demonstrated an epidural hematoma extending from C1 to C5 level. It was hyper intense on both T1 and T2 weighted images [Figure - 1]A and B. Coagulation profile done included bleeding time 1 min 45 s, clotting time 4 min 15 s, prothrombin time control 15 s, patient 16 s, and platelet count of 2.35 lakhs. Heparin, aspirin, and clopidogrel were discontinued and patient was given intravenous 1 gm of methyprednisolone and surgery was planned. Within 24 h from onset of weakness power improved to grade 4/5 on right shoulder and it was decided to continue conservative management. Bladder symptoms resolved within 15 days. MRI and MR angiography were repeated [Figure - 2]A and B after 2 weeks, which showed significant resolution of hematoma without evidence of arterial dissection. Chiropractic manipulation rarely leads to SEH with incidence being unknown due to limited case reports in literature.[2] Few case reports suggest association with thrombolytic agents, heparin and oral anticoagulants.[3] In our patient most likely the predisposing factor to SEH was uncontrolled hypertension and the same was accentuated due to chiropractic maneuvers and anticoagulants. Early decompressive laminectomy is advocated in patients with significant and progressive neurological deficit and constitutes the standard line of treatment. Conservative treatment according to one review may be limited to those patients who present with mild or no neurological impairment, early and fast improvement of neurological deficit within 24 h, or a small hematoma not compressing the spinal cord.[4] Methylprednisolone has been used occasionally with good results and its beneficial effects evolve around the membrane-stabilizing effect and the ability to suppress lipid perioxidation and hydrolysis and inflammatory chain reaction at the injury site.[5] References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06034f2.jpg] [ni06034f1.jpg] |
| |||||||||

{kind=link}
{kind=link}