 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
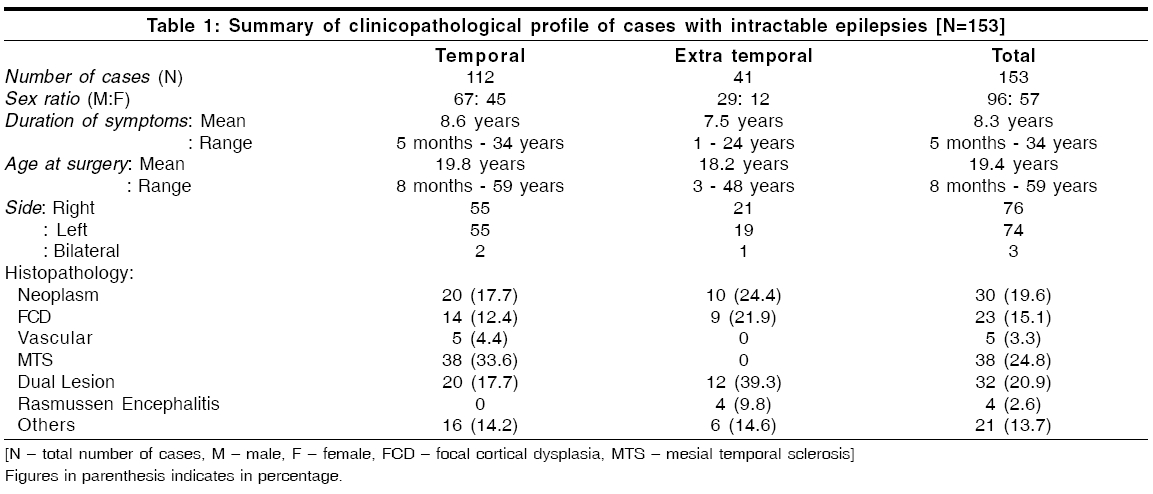
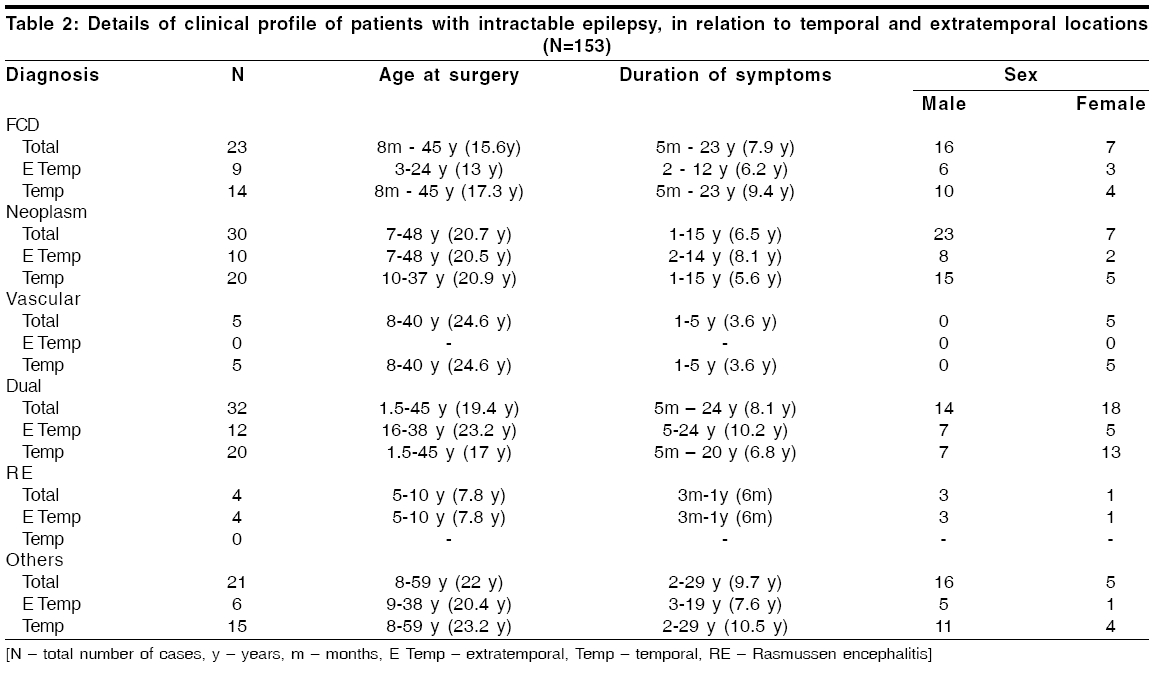
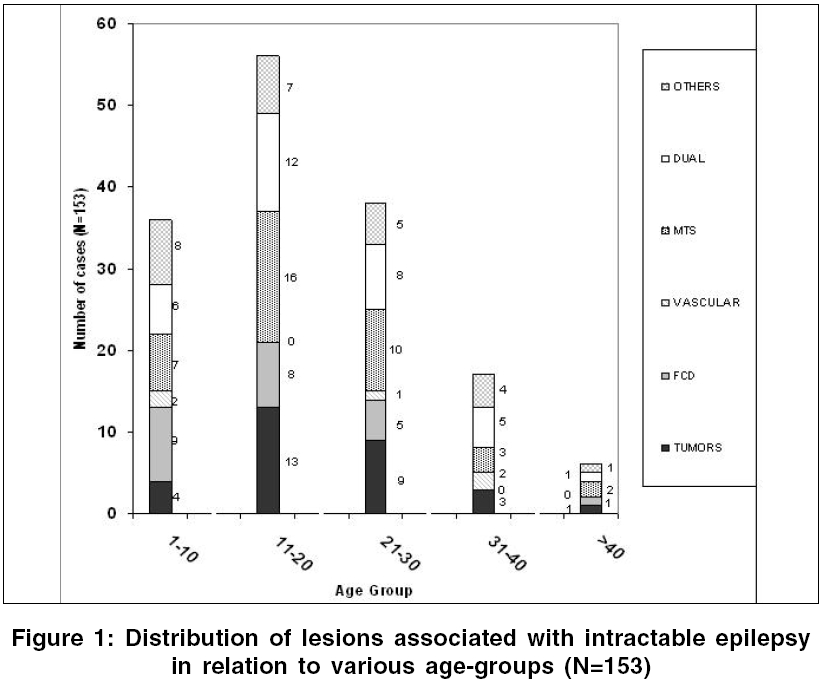
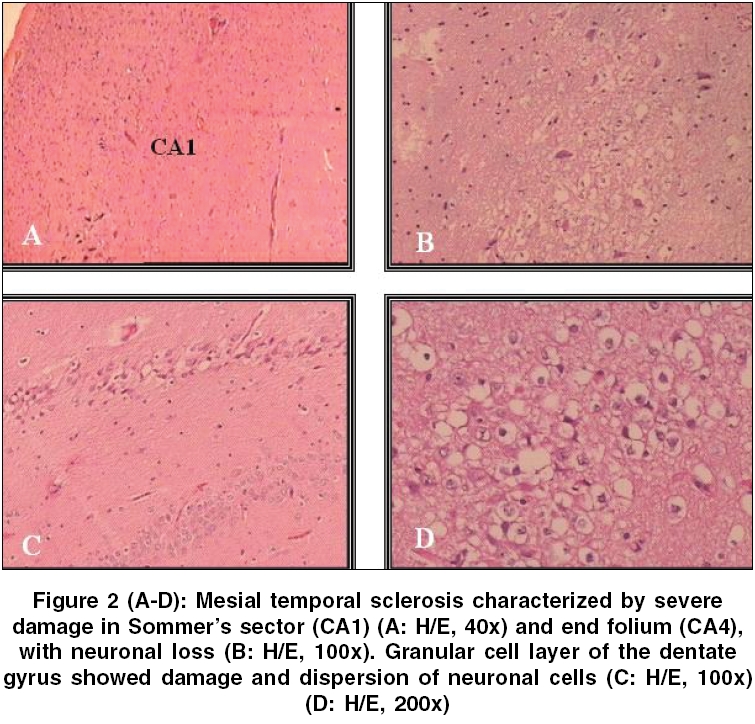
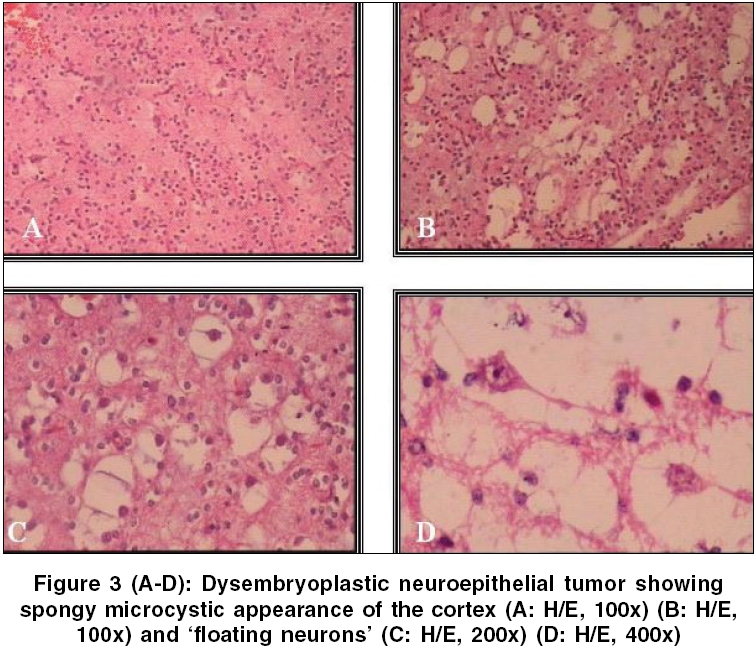
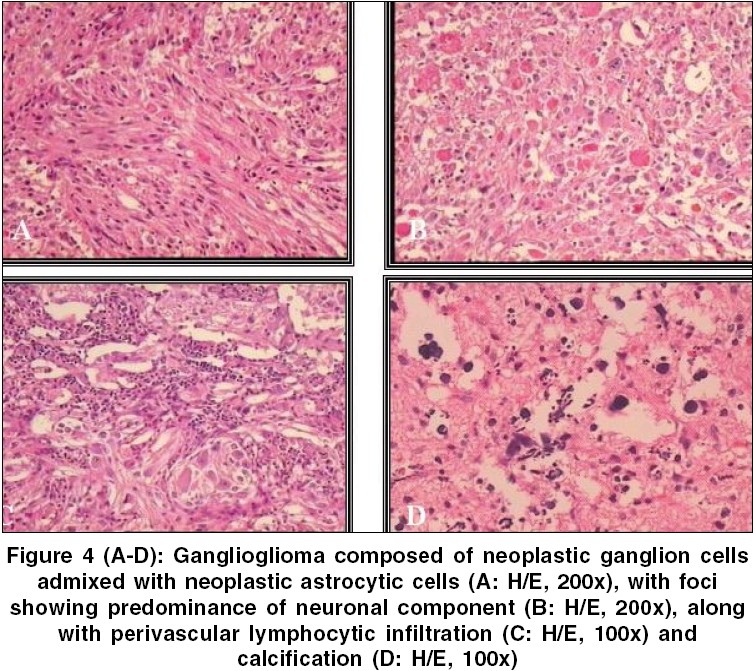
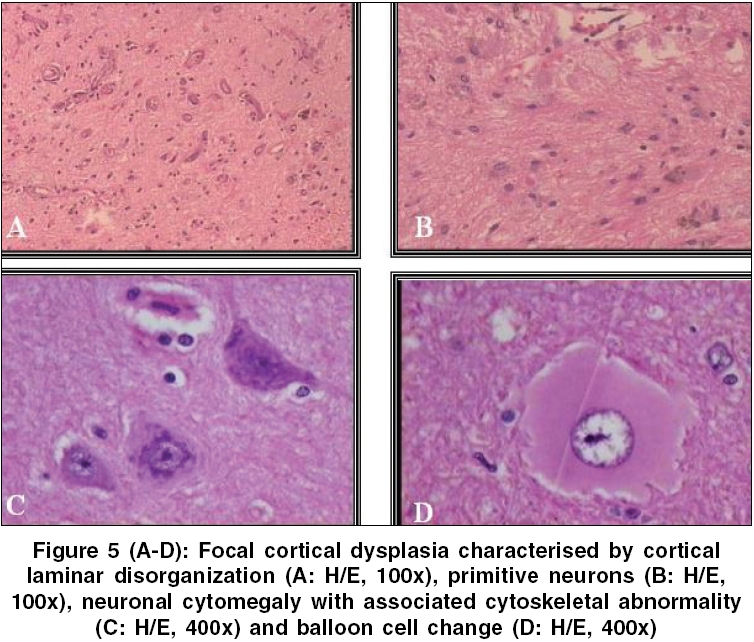
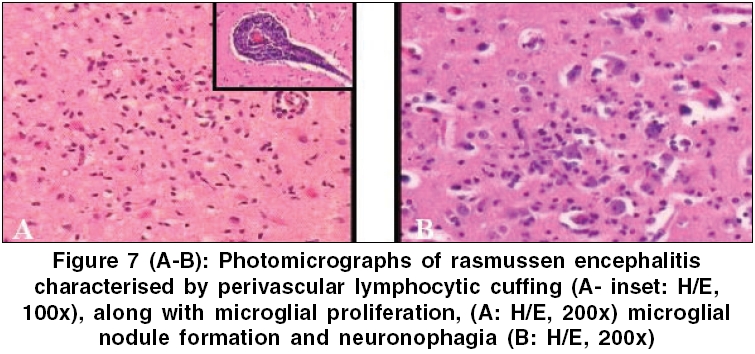
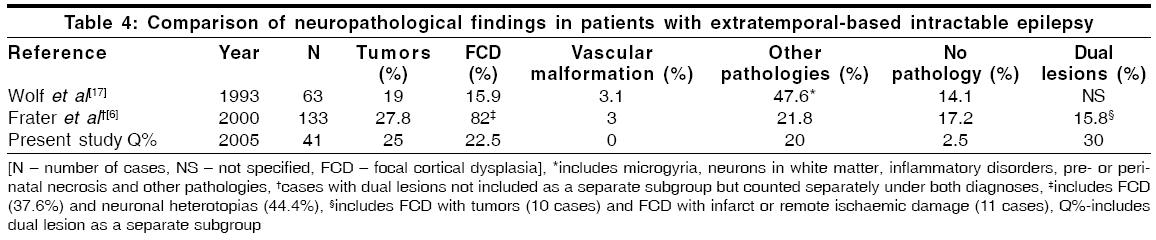
Neurology India, Vol. 54, No. 2, April-June, 2006, pp. 144-150 Original Article Neuropathological spectrum of lesions associated with intractable epilepsies: A 10-year experience with a series of 153 resections Sarkar Chitra, Sharma MeharChand, Deb Prabal, Singh VP, Chandra PSarat, Gupta Aditya, Tripathi Manjari, Bhatia Manvir, Gaikwad Shailesh, Bal CS, Jain Satish Departments of Pathology, All India Institute of Medical Sciences (AIIMS), New Delhi Code Number: ni06041 Related article: ni06042, ni06043 Abstract Background: Surgical management of intractable epilepsies is currently an established mode of therapy in various clinical settings.Aims: To retrospectively evaluate the neuropathological findings in both temporal and extratemporal lobe resections in such patients. Materials and Methods: The study included resected specimens from patients with intractable epilepsy managed at a tertiary care hospital of India, during a 10-year period (1995-2004). Results: A total of 153 patients, with mean age of 19.4 years and male predominance (73.2%) were included in the study. Overall, there was a predilection for the temporal lobe (73.2%), while 41cases were extratemporal in location. On histopathology, mesial temporal sclerosis (MTS) (24.8%) was the commonest lesion, followed by tumors (19.6%) and isolated focal cortical dysplasia (FCD - 15.11%). Other less common findings included Rasmussen encephalitis, non-specific gliosis and vascular malformations. In addition, 20.9% (32 cases) had dual lesions, majority of which included FCD with ganglioglioma (15 cases) or with dysembryoplastic neuroepithelial tumor (12 cases). In the temporal lobe, neoplasms and dual lesions formed the majority (apart from MTS), unlike dual lesions followed by neoplasms and FCD, in the extratemporal location. Conclusion: This series demonstrates that most patients with chronic intractable epilepsy have significant histopathological findings and highlights the neuropathological spectrum of such lesions, in the Indian context. This was similar to that reported from the West, but different from the single Indian series available in the literature. Further, the overall profile of temporal lobe lesions was not different from the extratemporal ones. Keywords: Intractable epilepsy, neuropathology, spectrum. Introduction Epilepsy is one of the commonest afflictions encountered in routine neurological practice, only second to stroke, in terms of incidence.[1] With the acceptance of surgery as an established and effective mode of therapy in epilepsy patients,[2] neuropathologists have an increasing opportunity to examine the surgical resection specimen and face the daunting challenge of explaining the importance of various structural abnormalities, in terms of seizure aetiology.[3]An overwhelming majority of these seizures originate in the temporal lobe,[4],[5],[6] owing to which the number of extratemporal resections in most epilepsy centers is relatively less as compared to temporal lobe surgeries.[6] Thus, series examining neuropathological profile in extratemporal-based chronic epilepsy have been significantly smaller. Surgical management of intractable epilepsy is currently restricted to few centres in India, which is reflected by the availability of only a single Indian series,[7] describing the pathology of underlying temporal lobe epilepsy. The present study was therefore undertaken to retrospectively evaluate the neuropathological findings in both temporal and extratemporal lobe resections in patients with drug-resistant epilepsy, managed at a large tertiary care neurosciences center in India. Materials and Methods This study comprised of surgically obtained specimens from patients with intractable seizures, managed at the Neurosciences Centre of this institute, between 1995 and 2004. Relevant clinical details viz. age at surgery, duration of symptoms, sex and site were noted. The seizure disorder was considered intractable if the patient had at least 2 seizures in a year despite an adequate trial of a combination of at least 2 first-line antiepileptic drugs at least for 2 years. This prompted an extensive presurgical evaluation consisting of electroencephalographs (EEGs), video-EEGs (short/long term), high-quality MR study using dedicated epilepsy sequences and MRS where appropriate, as well as interictal SPECT imaging (ictal when in doubt) and neuropsychological assessment. The surgical procedures performed were as appropriate to the location of the lesion, as well as the seizure focus identified intraoperatively on placing subdural grids during electrocorticography (Electroencephalograph 2100, Nihon Kohden Corp, Japan). In general, for temporal foci or lesions, a standard anteromedial temporal resection was carried out. For extratemporal lesions or foci, a tailored resection was performed including the morphologically abnormal area (to the extent feasible if location was in an eloquent area) and the area showing persistent "spikes" during intraoperative electrocorticography. None of the cases underwent a simple biopsy or non-resective surgery. In cases where further resection could not be done owing to the eloquent location of the seizure focus or pathology, multiple subpial transactions were performed. For patients with unilateral extensive foci, multilobar resections or functional hemispherotomy were considered. Patients with refractory drop attacks and having bilateral foci were considered for corpus callosotomy, while other patients with multiple bilateral foci were offered palliative procedures such as vagal nerve stimulation wherever appropriate. Histopathological evaluation Three pathologists (CS, MCS and PD) independently reviewed the slides. H&E slides along with relevant immunohistochemical stains [viz. glial fibrillary acidic protein (GFAP), synaptophysin, epithelial membrane antigen (EMA), synaptophysin, and neurofilament (NF)] were reviewed and the original histopathological diagnoses reconfirmed. Based on well-established diagnostic criteria, cases were classified into tumors,[8] focal cortical dysplasia (FCD),[9] vascular malformation,[10] mesial temporal sclerosis (MTS),[3] dual lesions and evidence of remote ischemic injury or infarct. Biopsies with co-existence of pathologies were termed dual lesions. Results Cumulative clinical profile A total of 153 consecutive chronic intractable epilepsy cases that were surgically treated during 1995-2004 were included, the clinical profile of which is elaborated in [Table - 1][Table - 2]. The spectrum consisted of 38 MTS, 30 neoplasms, 23 FCD, 5 vascular malformations, 4 Rasmussen encephalitis (RE) and 32 dual lesions. The other 21 cases included cysts, subpial gliosis, old haemorrhage and non-specific changes. The mean age at surgery was 19.5 years (range, 8 months-59 years), while mean duration of symptoms was 8.3 years (range, 5 months-34 years). Age at surgery in all subgroups of patients was comparable excepting FCD, where patients were younger (15.7 years) in age [Figure - 1]. Overall 87 cases (56.9%) were in the pediatric (≤ 18 years) age group. In general, male preponderance (M:F 1.7:1), with predilection for the temporal lobe (2.8:1) was observed. Extratemporal lesions were located in the frontal (17), parietal (15), frontoparietal (3), parietooccipital (2) and occipital (3) lobes. Seventy-six patients had right-sided lesion, in comparison to 74 with left-sided lesion, while in 3 cases it was bilateral. Mesial temporal sclerosis (MTS) MTS was the commonest lesion (24.8%), with a male predominance (1.7:1) and mean age at surgery and mean duration of symptoms of 24.6 years and 10.2 years, respectively. Nineteen were right-sided, while 17 were left-sided and 2 bilateral. All biopsies were characterized by severe damage in Sommer′s sector (CA1 and prosubiculum) and end folium (CA4 and hilus), with sparing of the subiculum and relatively resistant CA2. In addition, granular cell layer of the dentate gyrus displayed damage and dispersion of the neuronal cells [Figure - 2]A-D. Neoplasms Thirty tumors (19.6%) were diagnosed according to WHO (2000) criteria.[8] Mean age at surgery and mean symptomatic period were 20.7 years and 6.5 years, respectively. Left-sided predominance along with male preponderance was noted. The spectrum of neoplasms included dysembryoplastic neuroepithelial tumor (DNT) (14 cases), Ganglioglioma (GG) (6 cases), diffuse astrocytoma (4 cases), oligodendrogliomas (2 cases), oligoastrocytomas (2 cases), pilocytic astrocytoma (1 case) and pleomorphic xanthoastrocytoma (1 case). Twenty tumors were temporal in location, the profile of which, in terms of age at surgery and male predominance, were comparable with their extratemporal counterparts. However, temporal tumors were commonly on the left side and had a lower mean symptomatic period. Histologically, DNTs were benign cortical glioneuronal neoplasms, with small oligodendroglial-like cells arranged in a columnar configuration perpendicular to the cortical surface, between which neurons appeared to float in a pale, eosinophilic matrix (′floating neurons′ ), along with scattered GFAP-immunoreactive stellate astrocytes [Figure - 3]A-D. GGs were histologically characterised by neoplastic ganglion cells admixed with neoplastic astrocytic cells, along with perivascular lymphocytic inflammation and calcification, without any necrosis or mitosis. None of the tumors showed significant cytological atypia, high mitotic index, microvascular or endothelial proliferation, or necrosis [Figure - 4]A-D. Focal cortical dysplasia (FCD) FCD was identified in 23 cases (15.1%), with mean duration of symptoms of 7.9 years. These had male predominance, without predilection for any side. However, FCD had a lower mean age at surgery (15.6 years) in comparison to the others (overall mean 19.4 years). Temporal location was seen in 14 cases, the sex distribution and duration of symptom patterns of which were comparable to the extratemporal FCDs. However, the latter showed a younger mean age at surgery, with preference for the left side. FCD was defined as cortical maldevelopment in relation to the neuronal components. They were diagnosed based on the criteria suggested by Palmini et al ,[9] viz. cortical laminar disorganization, single heterotopic white-matter neurons or clustered neuronal heterotopia, neurons in the neocortical molecular layer, persistent remnant of the subpial granular layer, neuronal cytomegaly with associated cytoskeletal abnormality and balloon cell change (2 cases) [Figure - 5]A-D. Vascular malformation Vascular malformations were identified as per the guidelines suggested by Burger and Scheithauer[10] [Figure - 6]A-B. All were females with temporal-lobe lesions, displaying predilection for the left side. Mean age at surgery and mean duration of symptom were 24.6 years and 3.6 years, respectively. Dual lesions Thirty-two (20.9%) specimens showed dual lesions, majority (84%) of which were FCD with coexisting GG (15 cases) or DNT (12 cases), while the others were mesial temporal sclerosis (MTS) in conjunction with parasitic cysts (2 cases) and with cavernoma (1 case). In addition, there was one case of meningioangiomatosis with meningioma. This was histologically characterized by a transitional meningioma, in association with a cortical lesion showing numerous small intracortical blood vessels ensheathed by spindle shaped meningothelial cells and fibroblasts in cuffs and parallel bundles, imparting an ′onion-peel′ appearance. On IHC, the latter component was positive for EMA and vimentin, but negative for GFAP and S-100. Details have been documented in an earlier publication.[11] Mean age of dual lesions was 19.4 years, with mean duration of symptoms of 8.1 years. Overall there was female predominance, with predilection for the right hemisphere. Patients with temporal lesions were younger in age, had shorter duration of symptoms and affected the right side slightly more frequently than extratemporal lesions. Rasmussen encephalitis Four cases were of Rasmussen encephalitis (RE), which were marked by meningeal thickening, cortical atrophy with neuronal loss and reactive astrocytosis, perivascular lymphocytic cuffing, microglial nodule formation and neuronophagia and were sub-divided into broad groups, as suggested by Robitaille et al ,[12] viz. "active disease" (2 cases), " active and remote disease" (1 case) and "remote disease" (1 case) [Figure - 7]A-B. All four cases were extratemporal in location, affecting the frontal and frontoparietal lobes in 2 cases each. Mean age at surgery was 7.8 years, with mean duration of symptoms of 6 months and a male preponderance. Details of this series are available in an earlier publication.[13] Others Other less common, yet significant findings in terms of causative aetiologies of seizures included subpial gliosis (11 cases), old haemorrhage (3 cases), non-specific changes (2 cases) and parasitic cysts (1 case). Resection from 3 cases however did not reveal any anomalies but showed only normal white matter tissue. Discussion The present study included both temporal and extratemporal resections and endeavored in comparing their relative profiles with other similar studies.[5]-[7],[14],[15],[16],[17] Though, overall a temporal-lobe preference was noted, 26% cases had extratemporal involvement, with preference for the frontal lobe, which was similar to the series of Wolf.[15],[17]In order to obviate any selection bias, all 153 consecutive intractable epilepsy patients who underwent surgical management, were included in the study. In the present study, the overall mean age at surgery in both temporal and extratemporal locations was comparable. Though it was akin (19-21years) to that mentioned in literature for temporal resections,[5],[7],[14],[15],[16] it differed for patients with extratemporal lesions (26-30 years).[6],[17] Interestingly, majority (56.9%) were pediatric (≤ 18 years) patients, a figure hitherto not observed by other series apart from Wolf et al .[17] Structural lesions identified in 98% biopsies was synchronous with series reporting temporal-lobe resections[5],[7],[14],[15],[16] [Table - 3], but was marginally higher than that for extratemporal surgeries (82.8-85.7%) [Table - 4].[6],[17] This also highlights the fact that a larger number of normal-imaging cases can only be expected if there is an inherent selection bias during the presurgical evaluation to include many cases that were intensively investigated and found to have a concordant focus on electrophysiology and functional imaging, which was not the case in our series. Most large series reporting temporal-lobe resections[5],[15],[16] noted preponderance of tumors. In contrast, the current study observed a majority in MTS, akin to the series of Duncanl[14] and Radhakrishnan.[7] Though Duncan et al[14] noted dual lesions in 12.1% cases, their data included an overlap with 19 MTS cases and 8 non-specific hippocampal sclerosis. The study by Radhakrishnan group,[7] the only available Indian series, however consisted of very few neoplasms and no dual lesions. Frater et al[6] and Wolf et al[17] evaluated two of the largest series of extratemporal resections and observed malformative lesions, with preponderance of FCD, as the most common pathology as compared to tumors. Though the present study also revealed similar trend in terms of neoplasms, but overall dual lesions (30%) appeared to be the most frequent pathology, followed by FCD (22.5%). Though the 33.6% incidence of MTS noted in the current study appears synchronous with 22%-46.6% reported by other studies, it showed marked variation with the 62.3% incidence observed by the only other Indian series.[7] The latter series, contained very few neoplasms (6.2%), in comparison to literature,[5],[14],[15],[16] a feature which may possibly reflect selection bias. Neoplasms, encountered in around 20% cases, constituted the second most common pathology. Though this was similar to that observed by others,[6],[14],[15],[16],[17] it was distinctly different from the extremes of 56% and 6% noted by Plate et al[5] and Radhakrishnan et al[7] respectively. Majority of the neoplasms encountered in literature have been low-grade astrocytomas, GGs and DNTs.[18] However, few[19] noted WHO grade III / IV tumors, a feature not observed in the present study. In the current series, DNTs (46.7%) and GGs (20%) were predominant, which was similar (DNT: 64.9%; GG: 30.8%) to that noted by Pasquier et al .[16] Malformative lesions, comprising primarily of FCD, constituted a formidable group in most series[6],[15],[16],[17] including the present. This feature was prevalent more in extratemporal locations,[5],[6],[7],[14],[17] owing to the frequent involvement of temporal lobe by MTS and tumors. The wide variation between the FCD incidence noted by Wolf[17] and Frater[6] series [Table - 4] may possibly be explained by the definition used for cortical dysplasia, where glioneuronal hamartias included lesions composed of both glial and neuronal elements and were defined as "focal defect in tissue organization during development".[17] In the present study dual lesions had a high incidence (temporal: 17.7% and extratemporal: 30%) and was considered as a separate category. However, barring a few,[6],[14],[15],[16] others[5],[7],[17] have not considered this as a separate group. In temporal lobectomy specimens Duncan et al ,[4] Wolf et al[15] and Pasquier et al[16] observed dual lesions in 12%, 6% and 5.5% cases respectively, while Frater et al[6] noted coexistent pathologies in a significant minority (15.8%) of their extratemporal cases. The most common epilepsy-associated dual lesions, reported in the literature, included GG, glioneuronal hamartomas and DNTs.[20],[21],[22] Similarly, in this study, majority were dual pathologies of FCD in conjunction with GG or DNT. Interestingly, one case was that of an uncommon association of a rare entity, viz. meningioangiomatosis with meningioma, in a one and a half-year-old girl.[11] Literature pertaining to epilepsy-associated neoplasms, viz. GG and DNT, have observed an association with FCD, although the nature of this remains controversial.[6],[20],[21],[22] Whether these neoplasms arise from FCD, represent some peculiar forms of dysplasia, or merely coexist with dysplasia remains to be ascertained. In an endeavor to resolve this ambiguity, Blumcke et al[23] evaluated various seizure-associated glioneuronal neoplastic and malformative lesions and noted CD34-immunoreactivity in majority of GG and FCD (including dual lesions). Thus they proposed a common origin of these lesions from CD34-immunopositive bipotent precursor cells, which undergoes abnormal glioneuronal development.[24] This hypothesis was supported by colocalization of some of these cells with neuronal markers, like Neu-N and neurofilament[23] and immunopositivity for MAP-2 (cytoskeletal protein expressed in various neuronal and glial neoplasms, as well as in the developing nervous system).[25],[26] The less frequently observed findings in this series included vascular malformations, Rasmussen encephalitis, subpial gliosis, evidence of old haemorrhage and non specific changes, which were similar to that observed by other workers.[5],[6],[7],[14],[15],[16],[17] In the Frater[6] and Wolf[17] series, 17.3 and 14.1% biopsies respectively, did not reveal any obvious pathologic findings to explain the epilepsy. Similar observations were noted in 1.9% cases of the present study, which was similar to the 2% reported by Plate et al .[5] This phenomenon is possibly a resultant of alterations at molecular level, or anomalies of synaptic organization or dendritic arborization contributing to epilepsy, rather than structural disorganization, thus rendering histopathological evaluations futile.[6] Further, possibilities of loss of tissue with microscopic anomalies due to ultrasonic aspiration or routine laboratory processing may indicate that the true incidence of structural lesions in intractable epilepsies may be even greater than the current statistics. To summarize, this study compiles the neuropathologic spectrum encountered among specimens obtained from both temporal lobe and extratemporal lobe-based resections, in the course of management of epilepsy patients. Considering the large number of dual lesions and the unexplained significance of an association between FCD and neoplasms, it is suggested that this group be investigated further, in order to establish the exact neurobiology of these lesions and confirm their aetiological profile. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06041t4.jpg] [ni06041f6.jpg] [ni06041f5.jpg] [ni06041t3.jpg] [ni06041t2.jpg] [ni06041t1.jpg] [ni06041f4.jpg] [ni06041f1.jpg] [ni06041f2.jpg] [ni06041f7.jpg] [ni06041f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}