 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
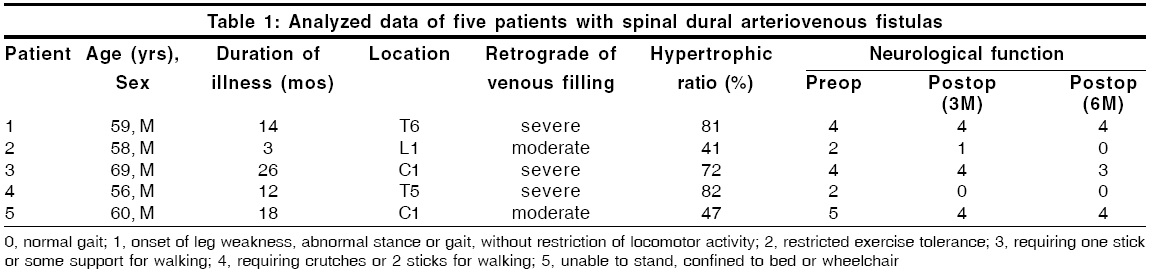
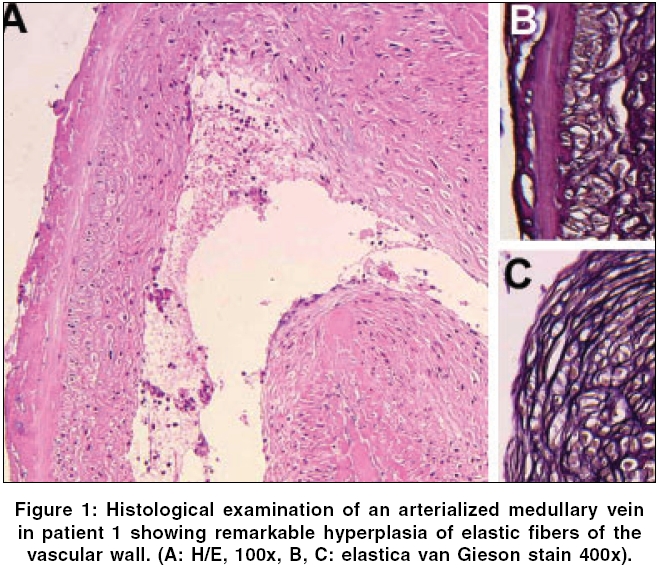
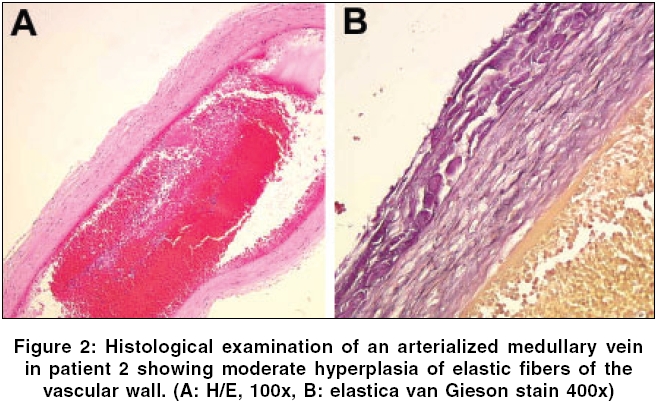
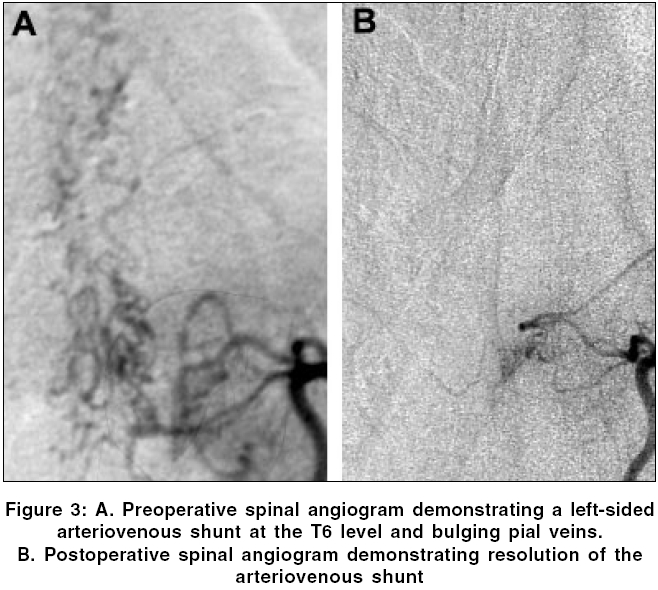
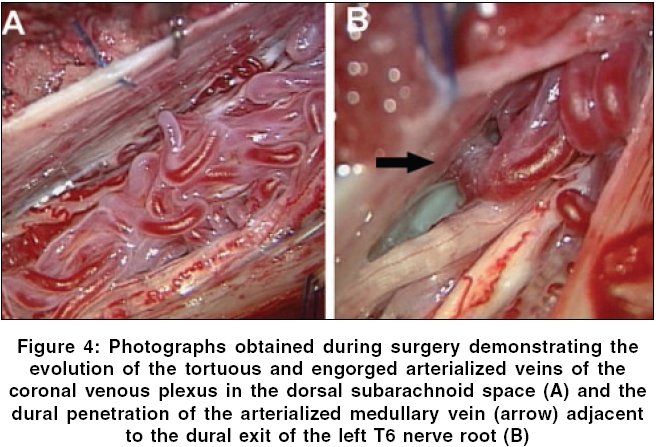
Neurology India, Vol. 54, No. 2, April-June, 2006, pp. 202-204 Case Report Histological characteristics of arterialized medullary vein in spinal dural arteriovenous fistulas related with clinical findings: Report of five cases Takami Toshihiro, Ohata Kenji, Nishio Akimasa, Hara Mitsuhiro Department of Neurosurgery, Osaka City University Graduate School of Medicine, Osaka Code Number: ni06060 Abstract The histological features of arterialized medullary vein (MV) in spinal dural arteriovenous fistulas (SDAVF) were studied in five consecutive patients who presented with progressive congestive myelopathy. Retrograde venous filling on preoperative angiography was recognized as being severe in 3 cases and moderate in 2 cases. Direct intradural interruption of the arterialized MV was performed in all patients. The arterialized MV was sampled and examined histologically to determine the percentage of the hyperplasia of venous wall (hypertrophic ratio). Histological examination of arterialized MV showed that hypertrophic alteration of venous wall structure was due to hyperplasia of elastic fibers, ranging from 41 to 82%. Patients with angiographically severe venous hypertension tended to have a higher hypertrophic ratio than patients with moderate venous hypertension. Our observations support the clinical concept that long-standing arterial stress in the spinal venous circulation causes histological alterations of spinal vascular structure associated with the progression of venous hypertension. We suggested that possibly the histological parameter can be used for predicting neurological recovery after occlusion of the fistulas.Keywords: Congestive myelopathy, medullary vein, spinal dural arteriovenous fistulas Introduction Spinal dural arteriovenous fistulas (SDAVF) are fed by a dural artery and drain directly into the valveless coronal venous plexus of the spinal cord via medullary vein (MV). The fistula can cause venous hypertension of the spinal cord, resulting in congestive myelopathy.[1],[2],[3] The basic strategy for treatment of SDAVF is interruption of the fistula.[1],[3] However, resolution of venous hypertension on MRI after treatment does not always lead to a functional recovery from SDAVF.[4],[5] This discrepancy between the resolution of venous hypertension and neurological recovery after treatment may be attributed to the progressive and irreversible nature or damage of spinal cord in SDAVF. We present five recent cases of SDAVF, which were treated by direct intradural interruption of the arterialized MV. Arterialized MV was coagulated electrically and transected at its origin close to the dura mater. A segment of arterialized MV was examined histologically to investigate the relationship between the spinal cord circulation and spinal cord function in SDAVF. Surgical technique to interrupt DAVF at the foramen magnum in Patient 3 and 5 was reported before.[6] Materials and Methods Five consecutive patients presented with progressive congestive myelopathy. MRI was conducted as the first diagnostic study and was followed by selective angiography. Our strategy for treating SDAVF was direct intradural interruption of the arterialized MV.[6] Retrograde venous hypertension was determined on preoperative angiography. Extensive and early filling of convoluted and tortuous veins of the coronal venous plexus with an arterialized MV was considered to be "severe" venous hypertension and early filling of the MV with minimal visualization of the coronal venous plexus was considered to be "moderate" venous hypertension. Gait function was scored before surgery and 3 and 6 months after surgery.[7] As a routine part of the surgical procedure, the arterialized MV was exposed intradurally and coagulated at its dural exit. A segment of the vessel was transected and sent for standard histological examination. Paraffin-embedded transverse sections of the vessel were analyzed after hematoxylin-eosin staining and elastica van Gieson staining in each case. A computerized image analysis system (microanalyzer, Nihon Poladigital, K.K, Japan) was used to determine the hypertrophic ratio of the arterialized MV (the percentage of the hyperplasia of venous wall). The total area as well as the lumen of the arterialized MV was determined. The hypertrophic ratio was expressed as a percentage by the following formula: (total area - lumen area /total area) x 100. Results Analyzed data of the five patients are summarized in [Table - 1]. Preoperative MRI showed extension of intramedullary high signal on T2-weighted MRI in all cases, suggesting the progression of venous hypertension. Degree of retrograde venous hypertension was graded as "severe" in Patients 1, 3 and 4 and "moderate" in Patients 2 and 5. Histologically, hypertrophic alterations of venous wall structure in arterialized MV varied among the patients, but were attributed to hyperplasia of elastic fibers [Figure - 1][Figure - 2]. The hypertrophic ratio varied among patients, ranging from 41 to 82%. Patients with severe venous hypertension tended to have a higher hypertrophic ratio than patients with moderate venous hypertension. Neurologically, all patients were stabilized or improved after surgery, with a gradual resolution (months to year) of spinal intramedullary high signal on T2-weighted MRI. Representative case This 59-year-old male (Patient 1) presented with a 14-month history of a gradually progressive gait disturbance and severe dysesthesia in the both lower limbs and up to the midthoracic level. His gait score was 4. Preoperative T2-weighted MRI demonstrated extension of intramedullary high signal up to mid-thoracic level. Spinal angiography confirmed extrinsic feeding vessels to dural fistulas and an intradural arterialized MV at T6 level, with early filling of convoluted and tortuous veins of the coronal venous plexus and an arterialized MV [Figure - 3]A. Thoracic laminectomy exposed large tortuous and convoluted veins in the subarachnoid space [Figure - 4]A. One of these veins was followed from the engorged coronal venous plexus to its site of dural penetration adjacent to the dural exit of the left T6 nerve root [Figure - 4]B, where it was ligated and resected for histological examination. This produced complete collapse of the engorged vessels of the coronal venous plexus. Postoperative spinal angiography confirmed complete obliteration of the SDAVF [Figure - 3]B. Two weeks after surgery, he experienced some improvement in sensory function, but the gait scores at 3 and 6 months after surgery were equal to the gait score before surgery. Discussion Surgical treatment of SDAVFs involves simple intradural interruption of arterialized MV, eliminating retrograde blood flow to the spinal cord, which halts the progression of congestive myelopathy. However, the postoperative course of neurological function does not always correlate with the reduction of intramedullary high signals on T2-weighted images.[4],[5] Several prognostic factors for functional recovery from SDAVF, such as age, duration of illness and neurological status just before treatment have been identified.[8] The relationship between the chronological change of spinal cord circulation and function in SDAVF is complex and needs to be elucidated. Congestive myelopathy caused by SDAVF, referred to as subacute necrotizing myelopathy, has been believed to be identical with the condition first described by Foix and Alajouanine in 1926. However, the term "Foix-Alajouanine syndrome" for patients with spinal dural AVF seems to be of little practical use and cannot be referred strictly to as a synonym.[9] This clinical entity of "Foix-Alajouanine syndrome" has been considered to be the result of progressive vascular thrombosis resulting in a necrotic myelopathy in a patient with a spinal AV malformation. Acute or subacute progression of non-hemorrhagic infarction in a patient with SDAVF is caused by progressive venous congestion. Hurst et al reported the spinal cord pathology in a case of angiographically proven SDAVF.[10] They documented a subpial angiomatous collection of vessels with thickened walls, extensive vascular sclerosis and gliosis in the white matter parenchyma, patchy myelin loss and concomitant axonal loss, identical to non-hemorrhagic venous infarction of the spinal cord and supporting the underlying mechanism of congestive myelopathy. Venous hypertension is transmitted directly to the intrinsic veins of the spinal cord with a decrease in tissue perfusion and progressive hypoxia of the neural tissue, ultimately leading to irreversible spinal cord dysfunction. Increasing blood volume or arterial stress into the spinal venous circulation leads to the histological alterations of spinal vascular structure, although anatomical variations among the patients or the possible progression of venous thrombosis in SDAVF should be considered. Although there are a limited number of cases in the present report, it may be helpful to predict the functional prognosis after treatment based on the findings of MV histology, or retrograde venous filling on preoperative angiography. Our observations support the clinical concept that long-standing arterial stress in the spinal venous circulation in SDAVF causes histological alteration of the spinal vascular structure associated with the progression of venous hypertension. We suggested that possibly the histological parameter can be used for predicting neurological recovery after occlusion of the fistulas. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06060f1.jpg] [ni06060f4.jpg] [ni06060f3.jpg] [ni06060f2.jpg] [ni06060t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}