 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
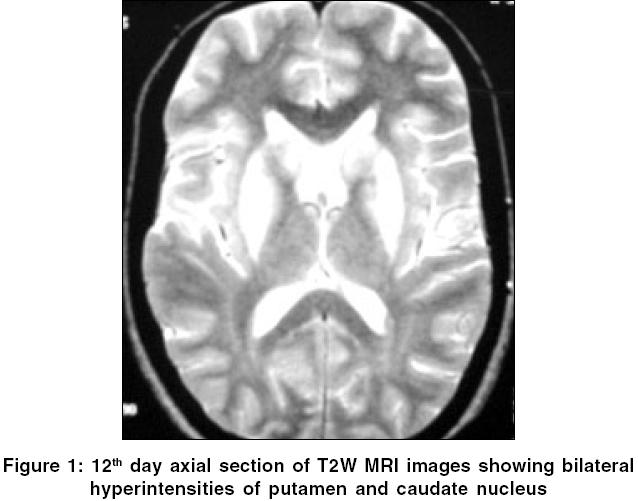
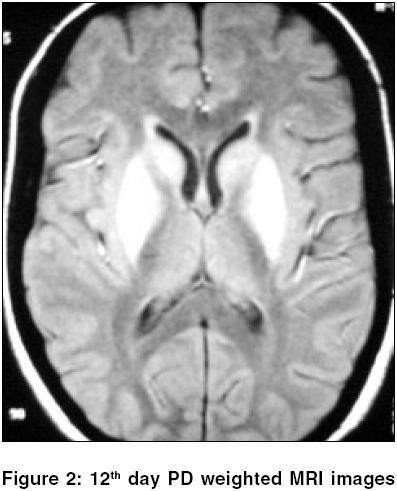
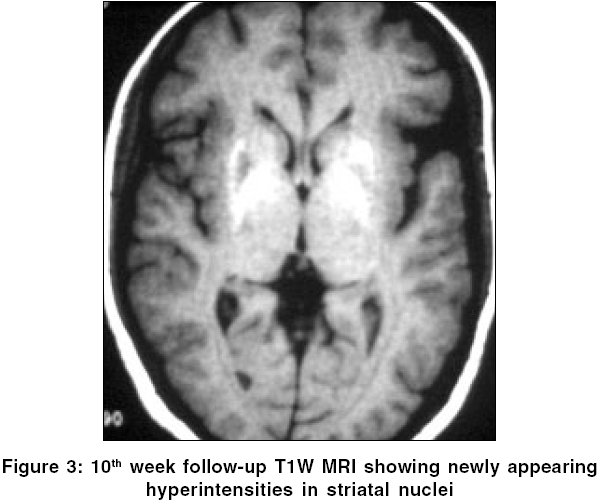
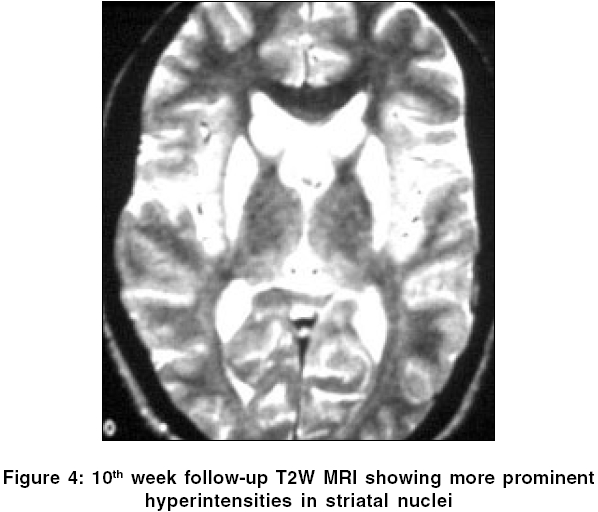
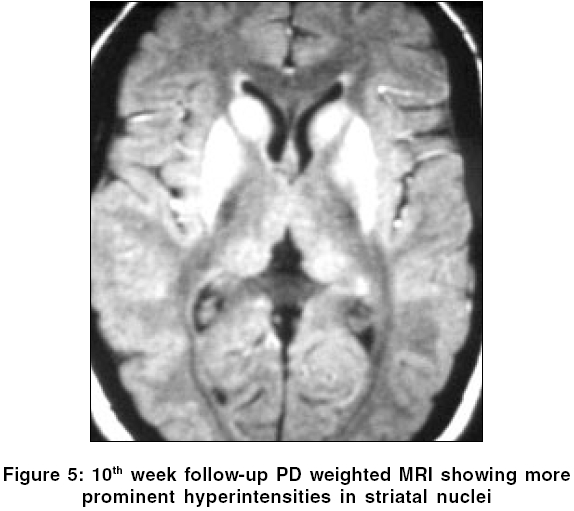
Neurology India, Vol. 54, No. 2, April-June, 2006, pp. 207-209 Case Report Magnetic resonance imaging changes in a case of extra-pyramidal syndrome after acute organophosphate poisoning Goel Deepak, Singhal Anil, Srivastav RajenderK, Verma Amit, Lamba Anurag Departments of Medicine, Himalayan Institute of Medical Sciences, Dehradun Code Number: ni06062 Abstract Distal symmetrical polyneuropathy and neuromuscular weakness is common neurological problem in recovery phase of acute organophosphate (OP) poisoning. Various types of extra pyramidal syndromes are uncommon sequel after OP poisoning. These are reported to be reversible within few weeks and characteristically associated with normal magnetic resonance imaging (MRI). In this report we are presenting a case with extra pyramidal syndrome after acute OP poisoning with few interesting MRI changes in striatum.Keywords: Parkinsonism, organophosphate, striatum, MRI, poisoning Introduction The acute muscarinic and nicotinic side effects of organophosphate (OP) poisoning are well known. After accidental or suicidal exposure, anticholinesterases lead to three well-defined neurological syndromes - that is, initial life threatening acute cholinergic crisis, intermediate syndrome with cranial nerve palsies, proximal muscle weakness and delayed organophosphate induced polyneuropathy. In addition to these three classical neurological syndromes following acute exposure and in some following low dose chronic exposure, several neurobehavioral changes have been observed and these have been termed together as "chronic organophosphate induced neuropsychiatric disorders" (COPIND).[1]Extra pyramidal syndrome (EPS) is uncommon intermediate neurological complication. This occurs after 4-40 days of intoxication and usually reversible within 8 weeks with or without treatment.[2] Neuroimaging was reported to be normal. We came across with a case of dichlorovos poisoning who had developed Parkinsonism on 10th day of acute poisoning with novel MRI abnormality in striatal nuclei. Case Report 21 years female admitted with history if self-deliberate heavy ingestion of pesticide (Nevon), which contains dichlorovos. She was unconscious and gasping due to massive dose, shifted to intensive care unit (ICU) for ventilator support and given atropine plus pralidoxime. Her blood pressure 110/70 mm Hg, heart rate 62/minute and temperature was 39°C. Second day patient regained consciousness and weaned off from respirator fifth day. On same day patient had psychotic behavior, thought to be due to atropine toxicity and was relieved with lower doses, without antipsychotic and shifted to general ward. During her short ICU stay she had not received total parental nutrition (TPN), except dextrose saline, additional gastric tube feeding was given from 3rd day onward. Next day she had vomiting and given single injection metoclopramide (perinorm). On 8th day atropine was stopped. On 10th day she started chewing movements, tonic unrolling of eyeballs, drooling of saliva and dystonic posturing of upper limbs. She had swallowing and speaking difficulty with episodic opisthotonic posturing. She had no significant past history of jaundice or other toxic exposure. On examination she had generalized pyramidal and extra pyramidal features with occulo-gyric crisis, tremor mask like face, hypophonia, cog wheeling, hypokinesia, postural instability and bilateral Babinski positive. K-F ring was negative on slit lamp examination. Laboratory studies were unremarkable except for white blood cell of 19600 cubic per mm. Liver function tests were normal, serum manganese level were not measured. Her cerebro spinal fluid (CSF) examination was normal. Magnetic resonance imaging (MRI) was done on 12th day with T1, T2 weighted and proton density (PD) images, showed symmetrical hyper intensities in Putamen and Caudate nucleus on PD and T2W images [Figure - 1][Figure - 2] and isointense on T1W images. Mid-brain, thalamus and cerebellum were normal. This patient responded well to dopamine agonist (bromocriptine) and trihexyphenidyl at discharge. Next week patient had severe axial dystonic movements, which improved after stopping bromocriptine. Follow-up magnetic resonance imaging (MRI) was done in 10th week (7th November) showed persistent and more prominent MRI changes on T2W and PD images, along with newly appearing hyperintensity on T1W images [Figure - 3][Figure - 4][Figure - 5]. Still this patient is having mild limb and perioral dyskinesia on trihexyphenidyl.Discussion Knowledge on EPS in acute OP poisoning is based on few case series. Davis et al first time in 1978 gave the idea that agricultural worker may be at risk of Parkinsonism due to chronic and repeated exposure to OP.[3] Commonest reported features in acute toxicity are oculogyric crisis and rigidity. First time Bhatt et al (1999) described typical Parkinson′s disease like manifestations with tremor, rigidity and hypokinesias in five cases with normal MRI in two patients and poor response to levodopa.[4] This is dose related (always with massive dose) and a self-limiting condition even without treatment. Re-exposure results in relapses. Few other have described the occurrence of a neuroleptic malignant syndrome during recovery from acute OP poisoning.[5] Dopamine agonists and amentadine were found to be useful in early treatment.[1]Few investigator had tried to find out focal abnormality in brain with single photon emission computed tomography (SPECT) and positron emission tomography (PET) however localizing MRI findings attributable to organophosphate poisoning have not been previously reported.[6] But in our case this was convincingly shown by localized and persistent MRI changes correlating with Parkinsonism and dystonia. Main differential diagnosis in our case for EPS can be direct toxic injury by OP, hypoxia, or drug induced. The absence of significant hypoxic insult and extrapyramidal symptoms after 5 days of normal neurological status on successful weaning from ventilator are points against hypoxic cause. Single shot of metochlopramide and MRI abnormality is unusual for drug induced EPS. Manganese toxicity was a possibility as MRI showing T1W hyperintensities but there was no history of exposure to manganese, as patient never had supplemented by TPN and no environmental factor, moreover worsening of MRI lesion in follow-up scan is unusual in this condition. These MRI changes are non-specific as many other metabolic and toxic conditions can produce similar changes. Groups of nuclei in Basal Ganglia (BG) are more susceptible to toxic injuries in absence of efficient detoxification pathway.[7] Due to high Iron content most of the BG nuclei (except Putamen and Caudate nucleus) appear as hypointense on T2W MRI in normal adults (second decade onward).[8] The differential diagnosis of symmetric abnormal signal in the basal ganglia is broad, including metabolic etiologies (mitochondrial disorders (Leigh), methylmalonic acidemia, Wilson′s disease, Hallervorden-Spatz), toxins (CO, methanol, cyanide) and hypoxic insult. Most of these disorders cause nonspecific T1 hypointensity/T2 hyperintensity with the exception of Hallervorden-Spatz. The pattern of symmetric T1 hyperintensity may be seen with calcification, TPN and liver disease.[9] Our case can be added as a rare cause of T1W hyperintensities in striatal nuclei on MRI after OP poisoning. Delayed appearance of T1W hyper intensities on MRI is interesting and can be explained either of the three basis, (i) selective binding of certain ions to the affected region as in manganese toxicity,[10] (ii) cellular swelling due to mitochondrial dysfunction as in cyanide poisoning[11] or presence of abundant gemistocytes (swollen astrocytes) at local site.[12] Combination of last two appears to be more appropriate for our case. Shortening of T1 relaxation time could result from the protein hydration layer inside the cytoplasm of swollen gemistocytes. Whether the condition with normal or abnormal MRI have different course is difficult to say on the basis of single case, as our case even with severe damage of striatum had fast clinical recovery with treatment. However these MRI abnormality and dystonic features after 2 months follow up indicate towards less benign course than previous reports. This report showing Extrapyramidal features and interesting MRI abnormality with severe OP poisoning supports the role of environmental toxins to cause various Extrapyramidal syndromes. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06062f1.jpg] [ni06062f3.jpg] [ni06062f5.jpg] [ni06062f2.jpg] [ni06062f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}