 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
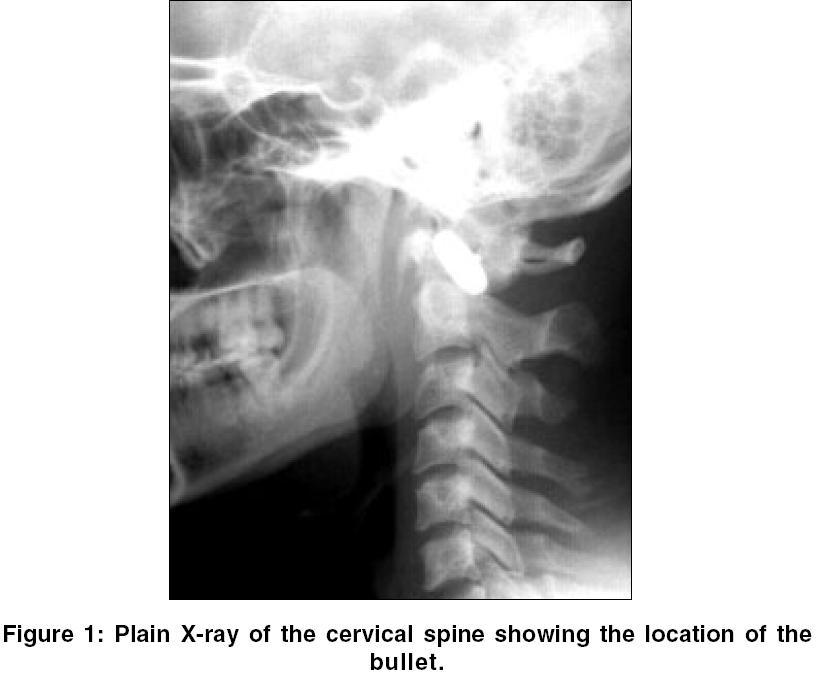
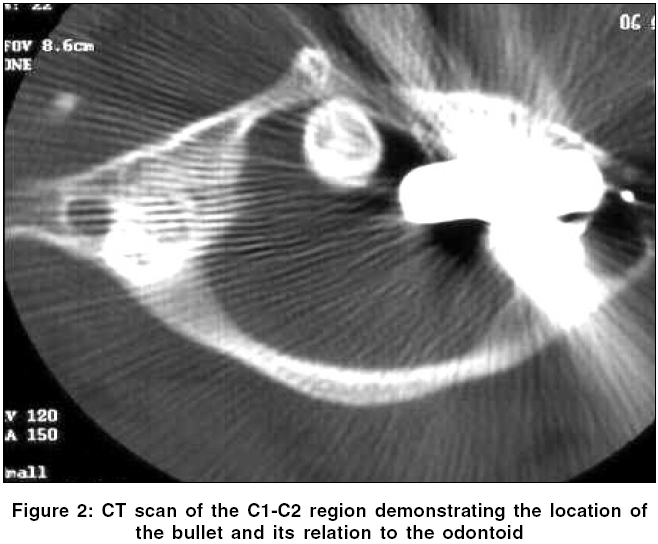
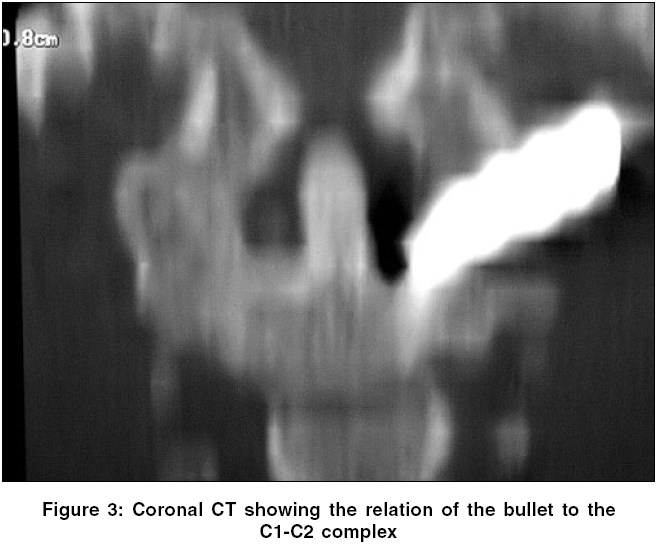
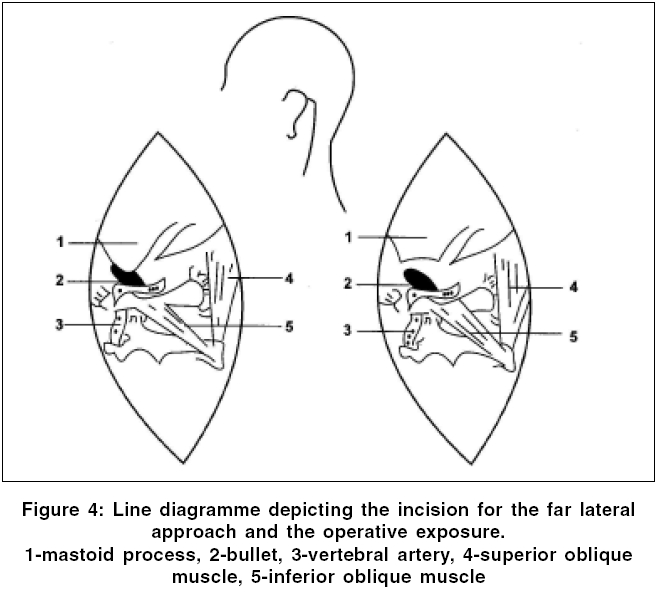
Neurology India, Vol. 54, No. 2, April-June, 2006, pp. 216-217 Letter To Editor Bullet injury to the atlanto-axial region Gupta SunilK, Gupta Sanjay, Bajaj Ajay, Mohindra Sandeep, Khosla VirendraK Department of Neurosurgery, Postgraduate Institute of Medical Education and Research, Chandigarh-160 012 Code Number: ni06067 Sir, Gunshot wounds (GSWs) of the atlanto-axial region are uncommon.[1] These injuries to the upper cervical spine are often devastating with loss of spinal cord function and respiratory compromise, sometimes leading to death.[2] A bullet penetrating the atlas without producing neurological deficits is exceptional.[3] A 21-year-old male was admitted with history of gunshot wound to the left side of neck 5 days before. Other than a left lower motor neuron facial palsy, there was no neurological deficit. An entry wound was present on left side of neck just below the mastoid. There was no exit wound. X-ray of the cervical spine showed a bullet in the region of C 1 vertebrae, posterior to the anterior arch [Figure - 1]. CT of the spine demonstrated that the bullet was lying obliquely behind the anterior arch of the atlas, about 3 mm from the odontoid [Figure - 2][Figure - 3]. Flexion and extension films of the cervical spine and craniovertebral junction did not demonstrate any mobility. Since the patient was neurologically intact with no evidence of any sensorimotor deficit, he was managed conservatively. However, about a week after admission, he started having pus discharge from the wound, which persisted despite antibiotics. A decision was therefore made to remove the bullet. A vertebral angiogram done prior to surgery showed that the vertebral artery was free from the bullet. The patient was operated through the far lateral approach. The mastoid bone and the sub-occipital triangle were exposed surgically [Figure - 4]. The bullet was hidden behind the mastoid process which was partially drilled off to visualize the bullet. The entry track of the bull et al so helped in its localization. The bullet was held with a Kocher′s forceps and lifted out without any resistance. There was no CSF leak, suggesting an intact dura. Postoperatively the patient did not have any additional neurological deficit. He was discharged on 8th postoperative day and has remained well in one-year follow up. Involvement of the axis has been reported in only 5% of all patients with GSWs of the cervical spine.[4] A bullet retained in the high cervical column without symptoms is highly unusual, though there are incidential such reports.[2],[5] The bullet was possibly low velocity and got lodged within the C 1 arch just adjacent to the odontoid process without causing any significant bony or neural injury. This type of presentation is extremely rare. The only absolute indication for surgical intervention has been reported to be the presence of a progressive neurologic deficit.[1] Other relative indications for surgical intervention include debridement and decompression of the spinal canal, assessment of spinal injury, repair of dural violations to prevent CSF leak and meningitis, to achieve reduction in infective complications and spinal stabilization.[6] Some authors[5] have reported that retained bullets did not increases the likelihood of septic complications while others advise[2] early removal to prevent septic complications. In the present case, development of local infection after one week and persistence of pus discharge despite antibiotics cover, led to surgical intervention for removal of the retained bullet . The surgical approach depends upon the site of entry and location of the bullet. In the present case, the entry wound was on the side of neck, below the mastoid and the bullet was near the left facet joints, posterior to the anterior arch, which was intact. The far lateral approach just followed the track of the bullet from the entry point. There was no need for any bony removal of the C 1 -C 2 complex. On the other hand transoral route necessitates bony removal which may have lead to instability in this patient. In patients with GSW of the C 1 -C 2 complex, flexion-extension studies to assess stability are required and may indicate the need for either external or internal stabilization. The indication of surgical intervention in the present case was the development of infective complication. Removal of the bullet was a surgical challenge; its removal led to rapid resolution of the infection with no perioperative morbidity. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06067f3.jpg] [ni06067f4.jpg] [ni06067f2.jpg] [ni06067f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}