 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
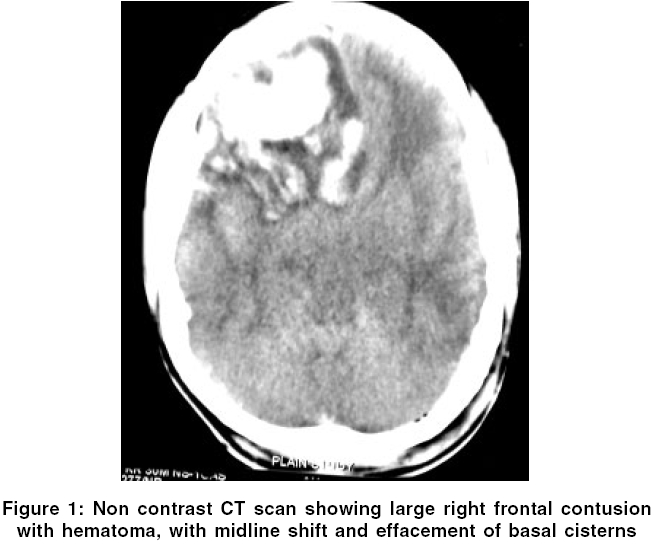
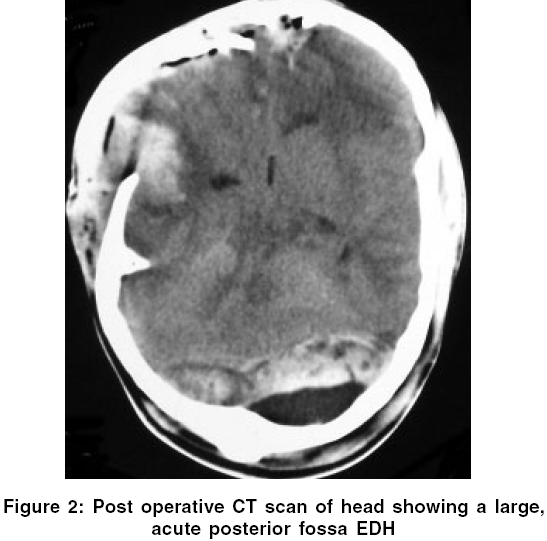
Neurology India, Vol. 54, No. 2, April-June, 2006, pp. 219-220 Letter To Editor Intraoperative development of posterior fossa extradural hematoma during evacuation of frontal contusion Faiz AhmadU, Mahapatra AshokK Cukurova University School of Medicine, Deparment of Neurology, Adana Code Number: ni06070 Sir, A 26-year-old man, fell down from a flight of six stairs and became unconscious. Before being brought to the casualty, he has 2 episodes of vomiting. On examination, he was localizing to pain and opened eyes to painful stimulus. His right pupil was 4 mm and not reacting to light but his left pupil was normal. He had minimal left hemiparesis. Plain CT scan of head (done 8 hours after the injury) revealed a large right frontal contusion with significant midline shift [Figure - 1]. All the basal cisterns were effaced. He was immediately taken up for surgery and right frontal craniotomy and right frontal lobectomy was carried out. By the time duraplasty was being done, brain started bulging significantly and operative cavity got obliterated. During and before surgery, patient received mannitol and was hyperventilated. The wound was closed and he was taken for CT scan directly. Non-contrast CT head revealed a large acute posterior fossa extradural hematoma (PFEDH) with mass effect [Figure - 2]. The hematoma was evacuated by midline subocciptal craniectomy approach. There was an occipital bone fracture with a large underlying PFEDH (fracture hematoma). The hematoma was also going supratentorially. No specific bleeder could be identified. Patient remained in comatose state in the post-operative period, developed postoperative meningitis and died 2 weeks later. The intraoperative development of contralateral epidural hematoma (EDH) is rarely described in the past.[1],[2] It is defined as a hematoma, not present on initial CT scan, but develops on the contralateral side during the process of evacuation of an acute traumatic hematoma.[1] It is manifested most dramatically by severe brain displacement during or following the craniotomy after the dura is opened or tense duramater if dura is not opened. If these signs are not noted, patient develops immediate postoperative raised intracranial pressure (ICP) or clinical deterioration. This entity is slightly different from "delayed epidural hematoma", which is any EDH that develops after an initial CT scan shows no hematoma.[3] However, delayed EDH can develop at any time after the initial CT scan, especially if the initial CT scan is done early (within first few hours of injury) and osmotic dehydration, hyperventilation, CSF otorrhea/ rhinorrhea, hypovolemia or surgical decompression have been associated, alone or in combination, after the trauma.[3],[4],[5] Intraoperative EDH, in contrast, is a subcategory of delayed EDH, which develops primarily due to rapid loss of tamponade effect of the dura and skull during a craniotomy and manifests most dramatically as severe brain shift after the craniotomy.[1] When this occurs during a surgery, cerebral edema, cerebral hyperemia and acute contralateral hematoma should be suspected. If brain does not get relax after osmotic diuretics and mannitol, wound should be closed after attaining hemostasis (without replacing the bone flap) and immediate CT scan should be undertaken. If CT scan is not available, alternate option is exploratory burr holes, which can be made contralaterally (first over the fracture site) in the temporal, frontal and parietal locations (in that order).[1],[2] As shown by our case, posterior fossa burr holes are also indicated if there is an overlying fracture or other burr holes reveal no hematoma. To the best of our knowledge, intraoperative development of PFEDH is not reported in English literature. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06070f1.jpg] [ni06070f2.jpg] |
| |||||||||

{kind=link}
{kind=link}