 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
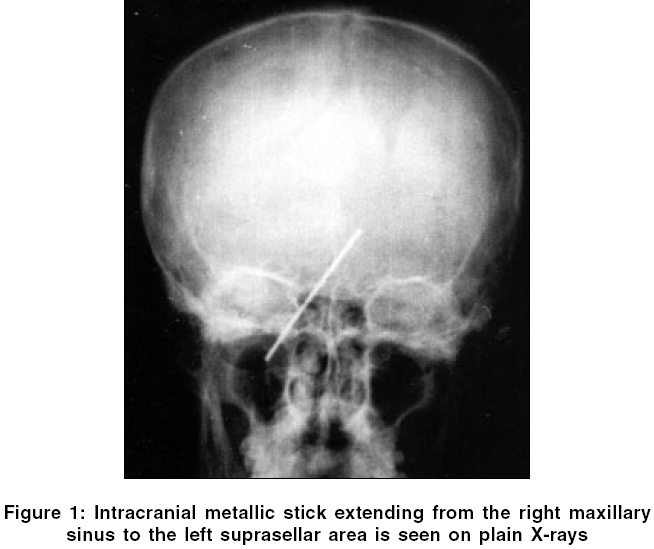
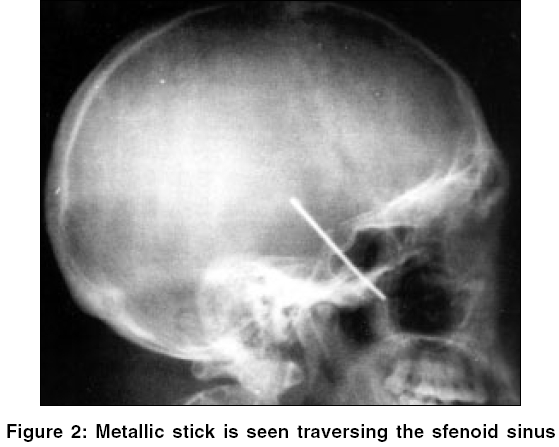
Neurology India, Vol. 54, No. 2, April-June, 2006, pp. 224-225 Neuroimage Intracranial metallic foreign body presenting with a unique route of introduction into the brain Sucu HasanK, Gelal Fazil Departments of Neurosurgery and Radiology, Atatürk Training and Research Hospital, Izmir Code Number: ni06074 A 29-year-old man, without any prior complaints, was admitted to our hospital after being kicked on his chin during a football game. He told that he had vomited for once after this minor head trauma and headache had developed subsequently. Neurologic examination disclosed a positive Achille clonus as well as positive Hoffman and Babinski signs on the right side. Plain X-rays and head computed tomography scan demonstrated a straight metallic stick, extending from the right maxillary sinus to the left suprasellar area and passing through the right sphenoid sinus [Figure - 1]. The stick was 7 cm in length, slightly thicker than a regular sewing needle and had rather blunted ends. The patient was not aware of how the stick had been introduced into his brain. He was brought up by his grandmother and remembered his grandmother′s telling him that he had fallen down the stairs with subsequent bleeding on his face and mouth, when he was a small child. The patient told that he was an amateur boxer. He did not experience vomiting or headache after the day of admittance. A surgical intervention was considered unnecessary and potentially harmful to the patient. On the follow up examination 3 years later, he did not have any complaints; Hoffman sign disappeared although Babinski sign persisted on the right side. Discussion The route of penetration of a foreign body can be judged by its position. For example sewing needles are usually inserted into the brain through open anterior fontanelle as a form of child abuse.[1],[2] Therefore, they are perpendicular to the cranial vault close to anterior fontanelle. In our case, it is evident from the X-ray findings that the stick did not penetrate through the fontanelle, cranial vault, orbits, nose or ear. The position of the stick, with the lower end in the maxillary sinus and the upper end away from the cranial vault, suggests that it was introduced intracranially through paranasal sinuses. We believe that the stick pierced his right lower cheek after he had fallen down and moved further intracranially traversing through maxillary and sphenoid sinuses [Figure - 2]. It is surprising that the stick had not caused significant injury in any of the vital and functional structures such as carotid arteries, cavernous sinuses, pituitary gland, or optic nerves; all of which are located in the area through which the stick had traversed.References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06074f3.jpg] [ni06074f1.jpg] [ni06074f2.jpg] |
| |||||||||

{kind=link}
{kind=link}