 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
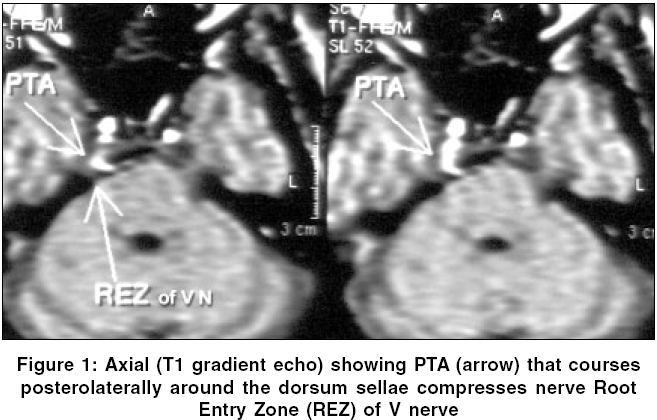
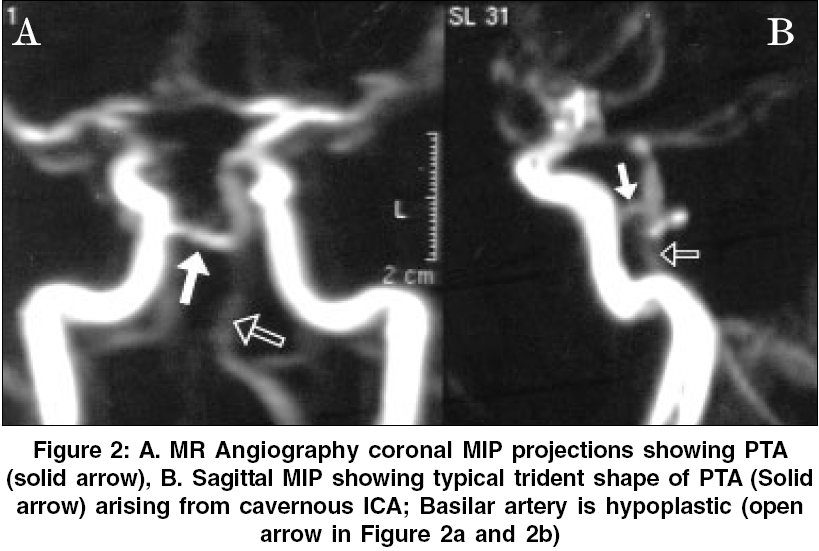
Neurology India, Vol. 54, No. 2, April-June, 2006, pp. 226-227 Neuroimage Persistent trigeminal artery: A rare cause of trigeminal neuralgia - MR imaging Chidambaranathan N, Sayeed ZaheerAhmed, Sunder K, Meera K Department of Radiology & Imaging Sciences, Apollo Hospitals,Chennai - 600 006 Code Number: ni06075 MR imaging (MRI) and MR Angiography (MRA) are useful in demonstrating vascular contact with trigeminal nerve at root entry zone (REZ) in-patients with trigeminal neuralgia.[1] Often a tortuous, ectatic superior cerebellar artery, vertebro-basilar or elongated antero-inferior cerebellar artery causes compression at the REZ.[1] Persistent trigeminal artery PTA (Primitive trigeminal artery) is a carotid basilar anastomotic vessel and documents itself in 0.02 to 0.6% of all cerebral angiograms.[2] A 48 yrs old male, presented with persistent pain on right side of face, of 2 years duration. The pain had increased along the distribution of V-1 and V-2 division of trigeminal nerve for the last 6 months. On examination no neurological deficit could be elicited. MRI (Sagittal T1, Axial T1 and T2 wt. Fast spin echo and high-resolution 3D T1 weighted gradient echo sequences) and MRA (using 3D TOF technique) were performed on a 0.5 Tesla MR unit. Maximum intensity projection (MIP) in three standard planes - axial, coronal and sagittal was generated. Thin slice reconstructed images were used to assess the fine anatomical relationship of the nerve and the vessels. MRI showed the origin of PTA to be arising from the postero-lateral aspect of the posterior bend of cavernous segment (C4) of right internal carotid artery (ICA), coursed postero-laterally and inferiorly around the dorsum sella and communicated with basilar artery in the prepontine cistern [Figure - 1]. In its lateral course, it compressed and distorted the REZ of right trigeminal nerve. As the patient was unwilling for micro-vascular decompression, he was treated conservatively with anti epileptic drugs. Discussion During fetal development (approximately 35 gestational days) the craniocerebral circulation is characterized by temporary connections between the primitive carotid and the paired dorsal longitudinal neural arteries (precursors of the vertebro-basilar system) appear. They include persistent trigeminal, ottic, hypoglossal and proatlantic intersegmental arteries. Normal embryonic development underwrites the regression of all these vessels totally. PTA is the most frequent (85%) of these primitive carotid -basilar anastomoses.[2],[3] Several anatomic variants of PTA have been described.[2] In this patient, the vertebro-basilar system distal to the anastomosis with PTA continued as contra lateral posterior cerebral artery. The ipsilateral posterior cerebral artery was supplied via patent posterior communication artery (PCoA). Basilar artery proximal to the anastomosis was hypoplastic and contralateral PCoA was absent. These findings are not in accordance with the previous discussions[3] but are in consonance with those described by Salaz et al .[4] These also include the sphenoidal (medial) variant documented with hyper prolactinemia arising out of compression of pituitary gland and stalk.[5] The petrosal (lateral) variant precipitates isolated VI nerve palsy. The instance under report is considered as a petrosal variant where the PTA compressed and distorted the nerve REZ of the trigeminal nerve, precipitating the facial pain syndrome. The other associations of PTA include aneurysm, internal carotid occlusions and vascular steal phenomena between basilar and carotid systems.[2] The identifying characters of PTA on MRI have been well documented.[2],[5] A proximal hypoplastic basilar trunk below the anastomosis that enlarges to a more normal caliber above the aberrant communication - an important ancillary sign of PTA was seen in this instance as well. MRA (sagittal MIP projection) displayed the trident shape of typical PTA arising from the cavernous ICA [Figure - 2]. The flow sensitive high resolution 3-D T 1 Wt gradient echo sequences rendered better depiction of the course of this aberrant vessel and the REZ, compared to the conventional spin echo techniques. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06075f2.jpg] [ni06075f1.jpg] |
| |||||||||

{kind=link}
{kind=link}