 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
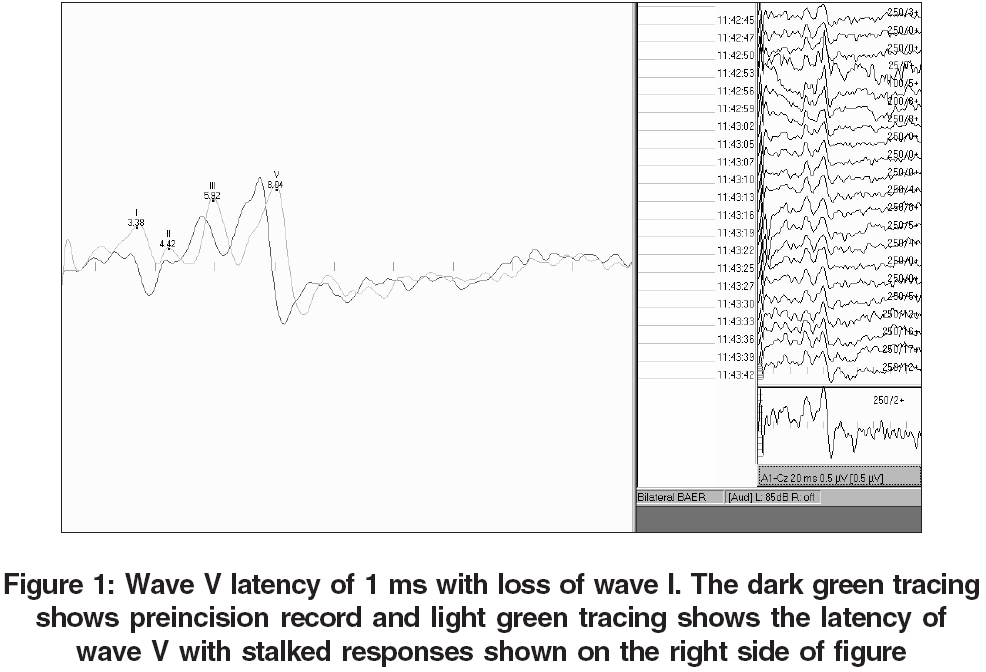
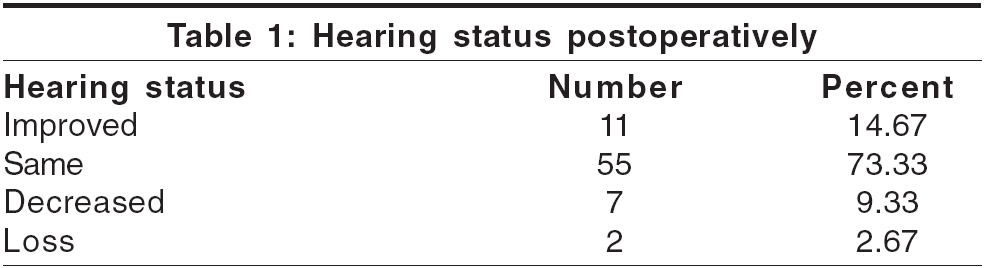
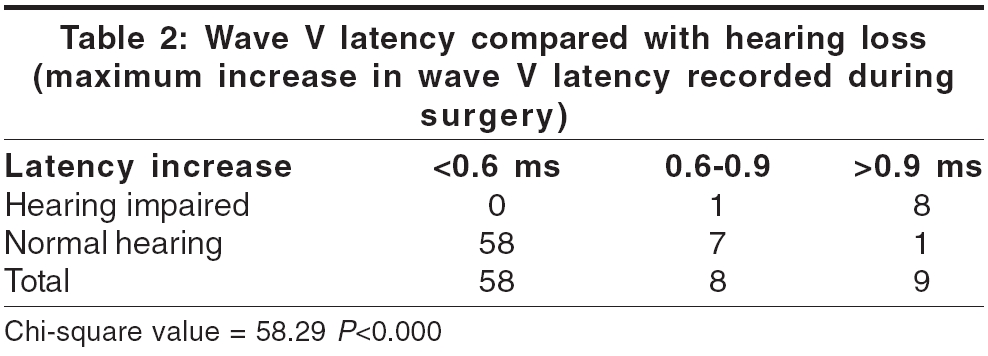
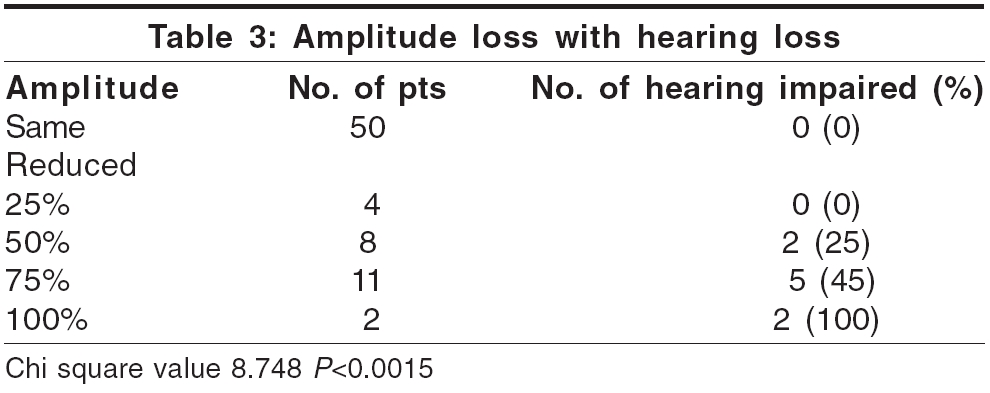
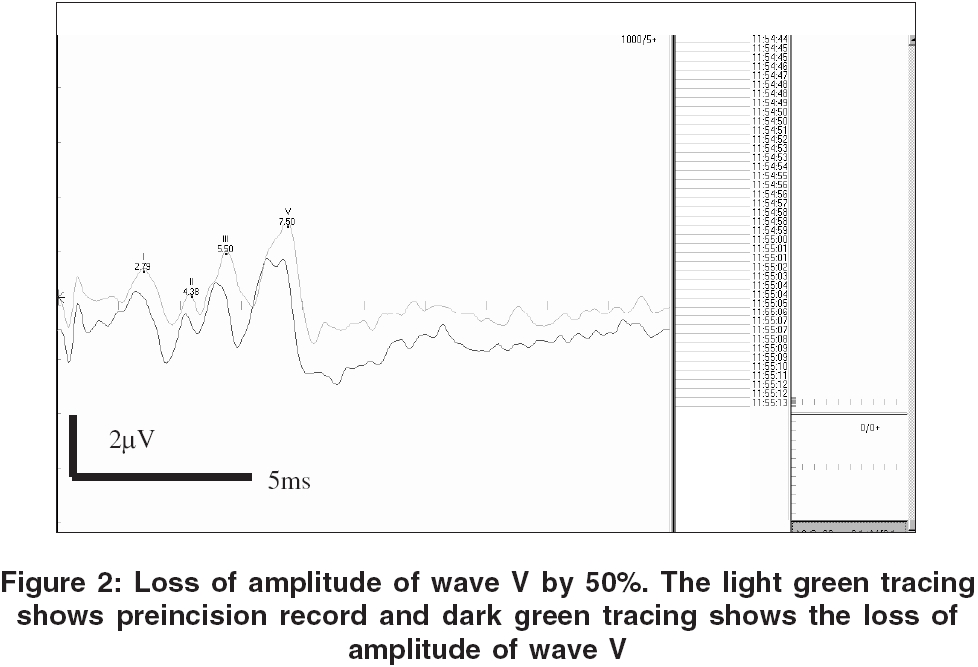
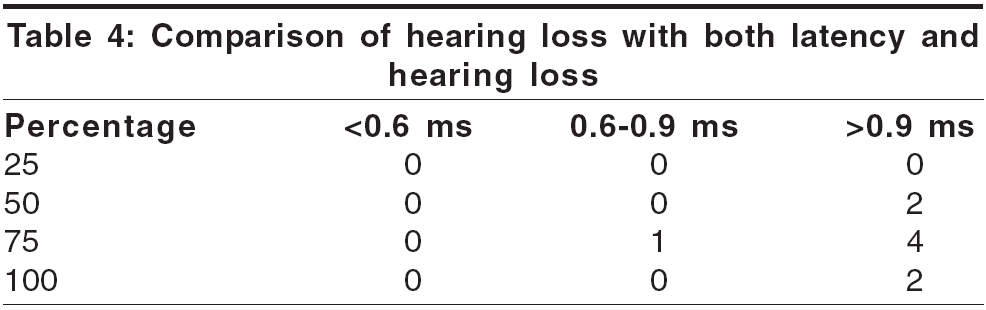
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 250-254 Original Article Brain-stem auditory evoked responses during microvascular decompression for trigeminal neuralgia: Predicting post-operative hearing loss Ramnarayan Ramachandran, Mackenzie Ian Departments of Neurosurgery and Neurophysiology, The Walton Center for Neurology and Neurosurgery, Liverpool, United Kingdom Date Accepted: 04-Aug-2006 Code Number: ni06083 Abstract Context: The importance of brainstem auditory evoked potential monitoring in reducing hearing loss during microvascular decompression for trigeminal neuralgia is now accepted. However the extent of the changes in the pattern of these potentials and the safe limits to which these changes are relevant in reducing postoperative hearing loss have not been established. Keywords: Hearing loss, microvascular decompression, trigeminal neuralgia, wave V latency Introduction Microvascular decompression (MVD) is a well-accepted treatment for trigeminal neuralgia (TGN). It is argued by many to be the treatment of choice, even in the elderly because of its high rate efficacy maintained in the long term.[1],[2],[3],[4],[5] Attention has rightly focused on the morbidity of the procedure, acknowledged to be greater than that of other treatment modalities. In particular, hearing loss is a recognized complication of MVD,[3],[6],[7] thought to be due to traction on the closely related auditory nerve. The integrity of the auditory nerve and to some extent the brainstem can be monitored per-operatively using brainstem auditory evoked potentials (BSAEP).[6],[7],[8],[9],[10],[11] Many studies have shown the effectiveness of intraoperative BSAEP monitoring in reducing hearing loss during MVD for TGN. [6],[7],[8],[9],[10],[11],[12] Some of these[8],[9],[11] have also shown the correlation of wave V latency with subsequent auditory outcome. Radtke[7] retrospectively compared the auditory morbidity of posterior fossa microvascular decompressive surgery before and after the introduction of intraoperative brainstem auditory evoked potentials. They concluded that a significant decrease in operative morbidity was directly associated with the use of intraoperative evoked potential monitoring. Raudzens and Shetter[11] concluded that BSAEP monitoring provided a good predictor of postoperative auditory status and may have prevented permanent neurological deficits in a small segment of patients by alerting the surgeon to potentially reversible abnormalities. Moller[10] suggested that intraoperative BSAEP monitoring has contributed to improvement in preservation of hearing during MVD. Some authors[8] have felt that the surgeon should only be made aware of the changes in evoked potentials that equal or exceed levels that may indicate permanent injury whereas others[10] opine that the surgeon should be informed about changes as soon as they become larger than the small variations that are normal for such potentials. Still some investigators[6] argue that the changes in BSAEP are not predictive of acoustic nerve damage as postoperative hearing is preserved. In this work, like that of others[10],[11],[12],[13],[14] loss of amplitude and increase in latency of wave V was considered to be the most important predictor of hearing impairment, but to date not much work has been done to quantify these changes and correlate it with subsequent hearing loss during MVD for TGN. In fact there is no clear consensus on the degree of latency shift and amplitude change necessary to represent a risk to later auditory function.[15] The objective of this study was to quantify the changes in the BSAEP during microvascular decompression for trigeminal neuralgia and to relate these changes to postoperative hearing impairments. Materials and Methods The policy of the unit is to offer MVD to patients with neurovascular compression demonstrated preoperatively by magnetic resonance imaging.[4],[16] All patients undergoing this procedure in our unit have BSAEP monitored during the operative procedure. Seventy-five such consecutive patients undergoing MVD for TGN due to vascular compression were assessed in this study. Preoperatively bilateral pure tone hearing thresholds across the frequency range 0.5 kHz to 8 KHz were established using a recently calibrated Kamplex AD40 audiometer with noise-excluding earphones. The audiometric assessments were standardized according to the American National Standards Institute. The patients were explained the tests in detail and all patients took part in the audiometry satisfactorily. Patients with severe pain or bandages had headphones applied to individual ears. BSAEP recordings were also standardized in all cases. The same investigator (IM) did all the audiograms and the brain stem evoked potentials. Nine patients out of a total of 84 who had preoperative ipsilateral hearing impairment or did not have a good audiogram were excluded from the study. The patients were induced with using a combination of propofol, ramifentanil and atracurium and maintained with sevoflurine and air mixture and positioned in the park bench position with the ipsilateral mastoid uppermost. Intraoperative monitoring of BSAEP was carried out using a Nicolet Spirit system (Nicolet Biomedical, Wisconsin). Three sub-dermal needles were placed for recording: the active electrode on the ipsilateral mastoid, reference at the vertex and earth applied to the forehead. Square wave click stimuli were applied using insert earphones at a frequency of 33.3 Hz and amplitude of 85 dB. Measurements were made preincision, prior to dural opening and from the time of dural opening until wound closure. The parameters analyzed for this study were the increase in latency and amplitude of wave V. Wave V can be detected even at near threshold levels and is normally found at 5.6 ± 0.23 ms.[4] Abnormal wave latency was defined as an increase in latency greater than 3 standard deviations over normal mean value (normal value 4.77 ms).[8] During surgery the surgeons are verbally told that latency is changing by having the responses stacked [Figure - 1]. Any change can then be seen appreciated easily. Often there is no magic figure but a trend or even just a slight increase each time becomes really apparent as compared to previous response because up to 16 waves are visualized on the screen at any one time. In the postoperative period all patients were asked about hearing at the bedside. None of the patients complained of any hearing loss. Pure tone audiometry was repeated (as preoperatively) 48 hours postoperatively and/or during the first follow-up visit and the average hearing threshold was tabulated. Tympanometry and otoscopy was done before the audiometry by an ENT surgeon (IM) to rule out any middle ear pathology. Only the information for the speech frequencies (1, 2 and 3 kHz) was used for the analysis. A change of 20 dBHL in the hearing threshold was taken as significant.[7],[12] All patients were followed up after three months and were asked about the hearing. Some patients (eight) mentioned that the hearing was probably slightly less in the operated side but was not a problem. These patients were then further tested by clinical as well as audiometry. Clinical assessment was done was done by whispering into each ear while masking the other ear. Audiometry was also done in all these patients as previously. Statistical analysis was done using the Chi-square tests. Results There were 75 patients in this study, 51 females and 24 males. The age ranged from 28 to 77 with an average of 55 years. The patients were divided into four groups based on the hearing postoperatively as compared to preoperative hearing. It was seen that 73% of our patients had no change in the hearing on the operated side and surprisingly about 15% had some improvement in ipsilateral hearing [Table - 1]. All patients (nine cases) with hearing loss had this on the ipsilateral side and all these were of sensorineural type. Interestingly, this hearing loss was not appreciated by the patients. It was seen that the clinical assessment of whispering was normal but the audiometry was definitely showing a drop suggestive of hearing loss. Wave V latency and postoperative hearing The increase in the latency of wave V was calculated as defined earlier. There was a correlation between peak latency increase and postoperative hearing deficit. It was seen that of the nine patients who had an increase in latency of wave V more than 0.9 ms, hearing impairment was seen in 89% [Table - 2]. In subjects with no change in hearing the average increase in the latency of wave V was 0.6 ms or less from the beginning to the end of the operation. Eight patients had an increase in the latency of wave V between 0.6 and 0.9 ms, which improved to base line by the end of the procedure. In this group only one patient had loss of hearing and she had an average wave V latency of 0.89 ms. It can be seen that increase in the latency of wave V was related to the hearing loss and this was statistically significant ( P < 0.000). The greatest increase in latency of wave V was seen when surgeons in training were operating (up to 2.17 ms). We had a mean displacement of 0.92 ms in our series. [Figure - 1] illustrates a case with wave V latency of about 1 ms. Wave V amplitude The amplitude of wave V per-operatively was compared to the hearing loss. From [Table - 3] it is seen that when amplitude loss was 50, about 25% of patients had hearing loss and this was progressive. But when this was 100% the hearing loss was 100%. This finding also was statistically significant ( P < 0.0015). It was observed that a break from retraction and surgery for a few minutes was usually associated with some recovery of both amplitude and latency changes. [Figure - 2] illustrates a case with loss of amplitude of wave V of about 50%. It was tried to separately analyze the correlation of hearing loss to increase in wave V latency of 0.9 ms or more and greater than 50% decrease in amplitude of wave V versus those in whom only one of these parameters was affected [Table - 4]. It is seen only in one case that when the amplitude was reduced by 75% did hearing loss noticed with increase in latency below 0.9 ms. In all other cases both amplitude and increase in latency of wave V seemed equally significant. However, meaningful correlation coefficients could not be worked out because of insufficient sample size. Discussion This study deals with brainstem evoked auditory potentials during microvascular decompression for trigeminal neuralgia and the relation of BSAEP to postoperative hearing loss. Audiometry has demonstrated abnormalities postoperatively with smaller intraoperative shifts in wave V latency than had previously been thought significant. It was seen that both increase in latency and decrease in amplitude of wave V were indicators suggestive of postoperative hearing loss. The importance of BSAEP monitoring in MVD has been clearly shown by many studies. [6],[7],[8],[9],[10],[11],[12],[13],[17] The latency of peak wave V has been considered the most important electrophysiological indicator for signaling auditory nerve damage by operative manipulations.[12],[14],[17] Broggi[6] had suggested that the abolition of wave V with preservation of wave I may be associated with good postoperative hearing function. Raudzens[11] noticed that intraoperative BSAEPs were unchanged throughout surgery in 34 patients (74%) and these individuals had no postoperative hearing deficits. Four patients had loss of all wave forms and this was correlated to deafness or hearing loss. They also felt that auditory morbidity had not declined with the increasing experience of the surgeon but it was seen in this series that this was not the case. Varying values of latency increase of wave V up to 1.5 ms have been to proposed to warn surgeons. Grundy[9] used a delay of latency of peak wave V of 1.5 ms to warn the surgeon by modeling on the warnings given in their previous experience. Radtke[7] chose latency changes equal to or greater than 1 ms to warn the surgeon. They commented that even though this value was chosen arbitrarily it was supported by the extremely low incidence of auditory complications seen in patients with shifts below this level. Hatayama[13] analysed patients with latency of peak wave V more than 1ms (38/350) and noted that 32% had postoperative hearing loss and felt that their results indicate that a latency change of more than 1ms poses a substantial risk of postoperative hearing loss. Similarly, when the amplitude of wave V was decreased below 40, 61% of cases had statistically significant hearing loss. They commented that the amplitude of the components of the BSAEP was more valuable than latencies and suggested that a decrease in the amplitude of wave V by more than 40% seems to be criterion for predicting postoperative hearing loss. However Friedmann[8] argued that false positive results will be frequent if latency criteria alone were used. They argued that as inter-peak latency was less affected by hypothermia, CSF drainage or depth of anesthesia, these are more sensitive to alterations secondary to surgical manipulations. They also suggested that simple prolongations of wave I, III and V latencies did not correlate with postoperative hearing deficit. They further suggested that notifying the surgeon regarding these prolongations may not be warranted. However, later studies have all felt the need for intraoperative BSAEP[4],[7],[10],[13],[14],[17] and warning the surgeon. Loiselle and Nuwer[18] commented that over reliance upon arbitrary warning criteria invites inaccuracy, which leads to increased patient risk. However, the concept of watching the BAEP waveform deteriorate until just prior to the disappearance of wave V before warning the surgeon does not seem acceptable. Most investigators[7],[11],[19],[20] have used empirically a 1.0 ms prolongation and greater than 50% decrease in amplitude of wave V as the criteria at which the surgeon has to be warned of impending damage. Polo et al[14] in a recent article on patients undergoing microvascular decompression for hemifacial spasm described as "critical warning" a delay of 1ms in the latency of peak wave V. In this series it was seen that both amplitude as well as latency change was significant but the latency increase was more so. They also noted that 9.5% of patients had no subjective decrease in hearing but laboratory examination showed hearing loss exceeding 20 db. In this series it was found that when the latency of wave V was more than 0.9 ms there was measurable hearing loss in 89% which was statistically significant. Regarding the amplitude it was seen that hearing loss was proportional to loss of amplitude above 50%. However, further correlating increase in latency and decrease in amplitude of wave V with hearing loss was not possible. Four patients (9%) in the Raudzens[11] series developed an abrupt ipsilateral loss of all waveform components beyond Wave I and had postoperative evidence of a pronounced hearing loss in the affected ear. Radtke[7] had three patients who had persistent loss of intraoperative BSAEP but only one of these patients had mild hearing loss suggestive of false positive result. Friedman[8] also had one similar case. In the study by Polo[14] there was a loss of hearing of 33.3% when wave V was abolished permanently. James[21] stated that commonly used warning values of a latency prolongation of 1.0 ms and amplitude decrement of 50% of wave V were not associated with hearing impairment. Using these warning values may needlessly prolong or alter the surgical procedure. The most important finding in this study is the fact of the hearing loss was not appreciated by the patient. Most patients after MVD do not complain when asked about hearing loss especially when done at the bedside. This is because the patient may be using the better ear for hearing. As mentioned earlier some of the cases were tested clinically as well as by audiometry. Many authors[14],[20] have pointed out about hearing being preserved even though wave V was lost. In normal clinical practice it is accepted that loss of wave V is a pointer towards hearing loss. But in our series this was found to be not true. In 11 patients (15%) of there was an improvement in ipsilateral hearing postoperatively. This was also noted in 7% of patients in one study.[7] There are several possible reasons for this: a) The retest phenomenon (the patient learns how to do the test). The one self-criticism of this study is that postoperative hearing loss was assessed very early. But middle ear assessments were also done to check that the loss was not conductive in nature. Also, with the improvement in current anesthesia techniques, patients become conscious and alert immediately and are discharged home by 48 hours. These patients can undergo audiometry very well in the immediate postoperative period. Patients were followed up in three months time and if there was any concern about hearing, patient was referred to the audiology department. Eight patients had audiometry repeated at that time. However it was noticed that this was not at all different from the record done at the immediate postoperative period. So it was felt that there was no reason to repeat the audiogram in all cases. This study came about as in our center it was assumed that after the wide use of BSAEP hearing loss was not an issue. But when the available information was viewed critically it was found that this was not the case. This paper highlights the problem of unilateral deafness after MVD not being observed by the patient. It also brings to focus the potential risk to patients having MVD on the side of their better hearing ear. It is suggested that patients who need to undergo MVD on the side of their better hearing ear need to be counseled that hearing could be compromised in that ear. Conclusions A per-operative increase in latency greater than 0.9 ms or a decrease in amplitude of wave V below 50% indicates a risk to hearing and should be indicated to the surgeon. The majority of these impairments may not manifest clinically.References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06083t1.jpg] [ni06083f2.jpg] [ni06083t2.jpg] [ni06083t4.jpg] [ni06083t3.jpg] [ni06083f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}