 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
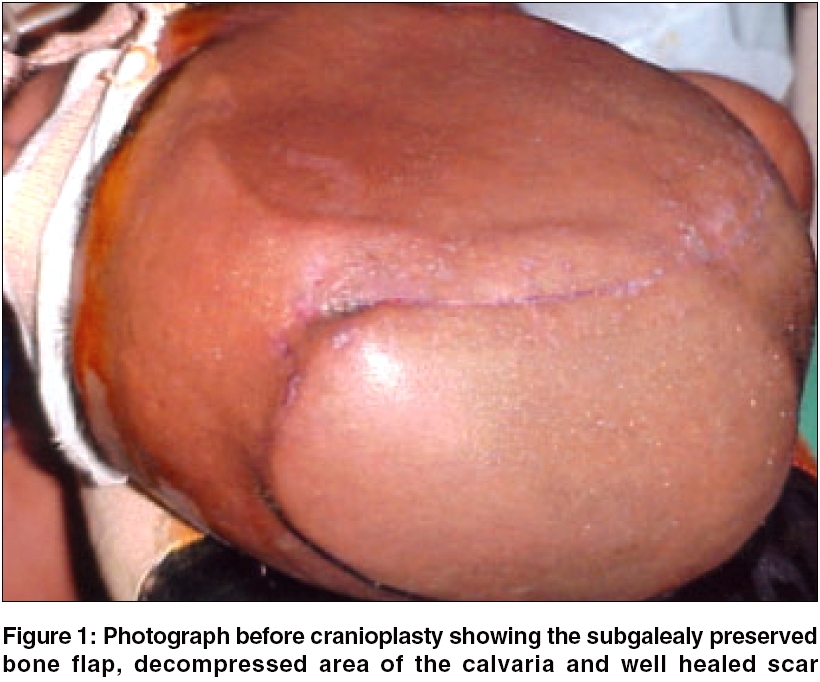
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 291-292 Technical Report Bone flap preservation after decompressive craniectomy- Experience with 55 cases Krishnan Prasad, Bhattacharyya AsisKumar, Sil Kaushik, De Rahul Department of Neurosurgery, National Neurosciences Centre, Kolkata - 700 031 Date of Acceptance: 25-Aug-2006 Code Number: ni06093 Abstract We describe our experience with the previously described technique of preservation of the bone flap in a subgaleal pocket created over the intact side of the calvaria, discuss our experience of this method and review the literature to compare this method with other alternative techniques. Key words: Bone flap, subgaleal pocket Introduction Decompressive craniectomy have a defined role in neurosurgical practice, especially in hemispheric stroke[1] and traumatic brain injury.[2],[3] Cranioplasty is done once the brain swelling subsides and the patient regains an acceptable functional status. Subgaleal preservation of the bone flap underneath the adjoining galea has been described earlier.[3],[4] We describe our experience with this technique.Materials and Methods We have prospectively analyzed 74 consecutively operated cases decompressive craniotomies done at the National Neurosciences Centre, Kolkata, over a period of two years (January, 2003 to December, 2004). Among them bone flap was preserved in the subgaleal pocket in 55 cases and in the subcutaneous tissue of the anterior abdominal wall in 9 cases. In the remaining 10 patients the bone flap was not preserved in vivo . Out of 55 patients where the bone flap was preserved in the subgaleal space, 49 underwent decompressive craniectomy for traumatic brain injuries. In 6 patients, craniectomies were done following removal of brain tumors (5 meningiomas, 1 intraventricular astrocytoma), where gross intraoperative brain swelling prevented primary bone closure. Surgical technique Following decompressive craniotomy, durotomy and evacuation of the clot, whenever indicated, a tissue pocket was created under the galea aponeuritica, in the immediate vicinity of the operative site, using a blunt dissecting instrument or by the surgeon′s fingers. The dissection extended generously to the contralateral side to create a space large enough to accommodate the bone flap. Strands of fibrous tissue were divided by sharp dissection with scissors. After the pocket had been developed, the bone flap was placed in such a manner that it conformed to the curvature of the scalp [Figure - 1]. Sharp edges of the bone flap were nibbled away to decrease the chance of necrosis of the overlying skin. We had managed to insert even very large fronto-temporo-parietal bone flaps by this technique. Large bifrontal bone flaps were divided in the middle before insertion. A vacuum drain was placed inside the pocket to prevent any subgaleal collection. During cranioplasty, after reopening the incision and defining the bone margins, the bone flap was pulled out of the subgaleal pocket and anchored to the margin of craniotomy defect. Results Average extra time required for subgaleal dissection was 16 minutes (range: 12-20 minutes) and average size of bone flap was 10 x 9 cms (range: 8-13 x 7-12 cms). The average duration of preservation before interval cranioplasty was 3 months (range: 6 weeks to 8 months). We encountered complications in two cases. In one, there was breakdown of part of the overlying skin due to a sharp spicule of bone inadvertently left projecting from the flap. Faulty creation of an inadequate pocket in comparison to the size of the bone flap led to the necrosis of the skin incision in the other patient. At the time of cranioplasty, done after a few months, we did not encounter macroscopic resorption of the bone flap in any of our patients.Discussions Bone flap can be replaced by artificial material, or by the patients own bone removed during the surgery. The alternative in vivo method described in the literature is preservation of the bone flap in the subcutaneous pocket of anterior abdominal wall.[5] The method of subgaleal preservation of the calvarial flap avoids an abdominal scar, maintains bone quality due to the relative avascularity of the subgaleal plane and is less time consuming than the abdominal preservation method. The technique has earlier been described in literature[3],[4],[5],[6] and all the previous authors have found it to be advantageous. We feel subgaleal preservation of patient′s own bone flap is a suitable, easy, cheap, sterile and histocompatible alternative with better physiological and cosmetic results than other techniques. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06093f1.jpg] |
| |||||||||

{kind=link}