 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
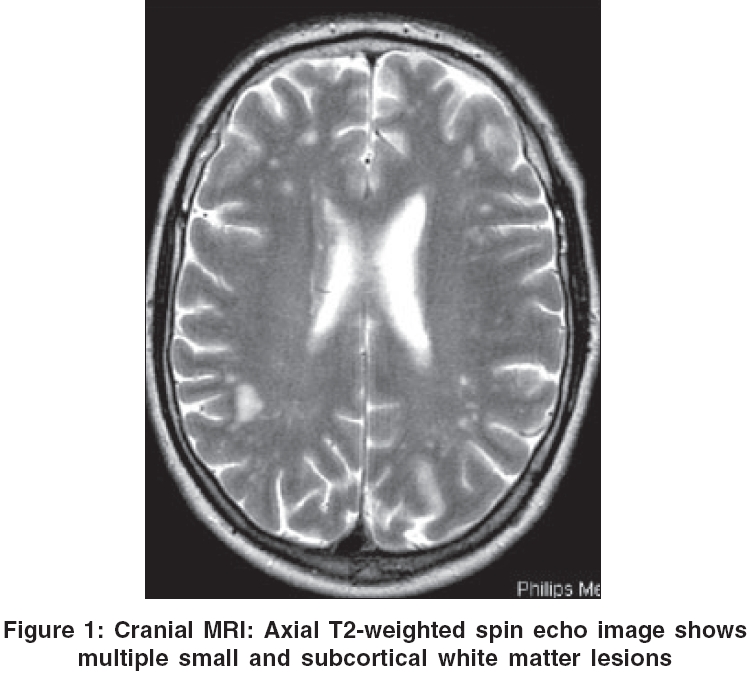
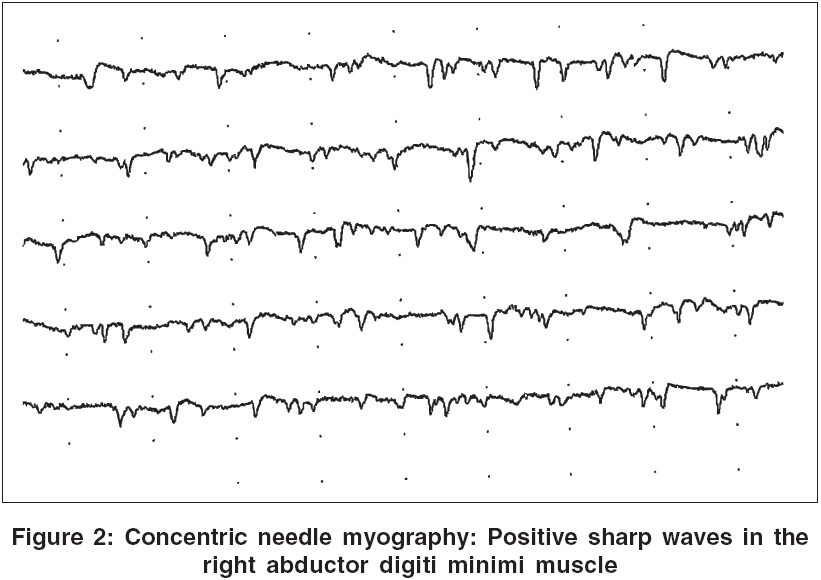
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 301-303 Case Report Hashimoto's encephalopathy and motor neuron disease: A common autoimmune pathogenesis? Harzheim Michael, Feucht Jeanine, Pauleit Dirk, Pöhlau Dieter Department of Neurology, Kamillus-Klinik, Asbach Date of Acceptance: 25-Aug-2006 Code Number: ni06097 Abstract Hashimoto's encephalopathy is a rare complication of autoimmune thyroiditis not associated with thyroidal function decline. We report a 50-year-old man presenting with lower motor neuron symptoms evolving over 3 years and changes in behavior associated with attentive and cognitive impairment occurring in the last few months. Memory deficits, emotional instability, marked dysarthria, mild symmetric weakness of the lower extremities, and fasciculations were the most striking clinical features. EEG was diffusely slow, cranial MRI revealed multiple subcortical white matter lesions, CSF protein was slightly elevated, electromyographic recordings showed acute and chronic denervation, and extremely high TPO antibody titers were found in the serum. Hashimoto's encephalopathy and lower motor neuron disease were diagnosed. As repeated high-dose intravenous methylprednisolone administration followed by oral tapering improved both central nervous system and lower motor neuron symptoms, the question was raised whether there was a common autoimmune pathogenesis of both clinically distinct diseases. Keywords: Corticosteroid therapy, hashimoto′s encephalopathy, motor neuron disease Introduction Hashimoto′s encephalopathy (HE) is a subacute, steroid-responsive, relapsing-remitting encephalopathy associated with Hashimoto′s thyroiditis, usually presenting with dementia, alteration of consciousness, stroke-like episodes and epileptic seizures.[1],[2],[3],[4] A comorbidity of HE and motor symptoms has been rarely reported. An association of multifocal motor neuropathy and asymptomatic Hashimoto′s thyroiditis in a 61-year-old man with a 2-year history of slowly progressive weakness with amyotrophy and fasciculations has been described first in 2002.[5] Neurographic recordings revealed multifocal motor conduction blocks, and laboratory tests demonstrated elevated anti-GM1 antibodies and Hashimoto′s thyroiditis. Another case of muscle weakness and atrophy due to multifocal motor conduction blocks and Hashimoto′s thyroiditis in a 17-year-old man has been reported 2 years later.[6] In addition, an association of lymphocytic thyroiditis and peripheral neuropathy in 6 of 53 cases and of lymphocytic thyroiditis and encephalopathy in 2 of 53 cases has been described in 1990.[7] Here we report a patient with cognitive impairment associated with a lower motor neuron disease, which coincided with extremely high serum titers of antithyroid peroxidase (TPO) antibodies.Case Report A 50-year-old man presented with chronic progressive dysarthria for 3 years paralleled by mild symmetric weakness of the lower extremities and diffuse fasciculations, but no muscle cramps. His wife reported the occurrence of aggressive behavior and memory deficits in the last few months. Besides smoking, there was no other vascular risk factor. Medical history, as well as family history, was negative for other symptoms or diseases. Clinical examination revealed emotional instability, memory deficits and marked dysarthria. In addition, monopedal hopping and walking on toes were impaired bilaterally and diffuse fasciculations could be observed at all extremities. Fasciculations of the tongue, amyotrophy, focal paresis, alterations of deep tendon reflexes, Babinski′s sign, and sensory deficits were absent. Laboratory examinations revealed extremely high serum titers of TPO antibodies (1063 U/ml) and elevated triglycerides. Further analysis of blood, including differential blood cell count, C-reactive protein, electrolytes, liver enzymes, creatinine, urea, glucose, serum protein, thyroidal hormones, antinuclear antibodies, antineutrophil antibodies, anti-GM1 antibodies, antithyroglobulin antibodies, thyroid stimulating immunoglobulins, CEA, and anti-Hu antibodies, was within the normal range. Cerebrospinal fluid (CSF) analysis showed a mild increase in protein content (0.58 g/l). Other CSF parameters, including opening pressure (18 cmH 2 O), cellularity, glucose content, determination of intrathecal IgG synthesis, and CSF oligoclonal bands by isoelectric focusing, were normal. Serological studies, including determination of serum and CSF antibodies against herpes simplex virus (HSV), varicella zoster virus (VZV), human immunodeficiency virus (HIV 1/2), mumps, measles, rubella, Treponema pallidum, and Borrelia burgdorferi, were normal. EEG was diffusely slow (7-8/s) without epileptiform or focal activity. Cranial magnetic resonance tomography (cMRI) detected multiple small signal alterations in the subcortical white matter in T2-weighted images without gadolinium enhancement in T1-weighted images [Figure - 1]. Concentric needle myography gave evidence of acute denervation with recording of fibrillation potentials, positive sharp waves, and fasciculations in the right biceps brachii, tibialis anterior, and left abductor digiti minimi muscles; and of chronic denervation with recording of prolonged duration or increased amplitudes of motor unit potentials in the right biceps brachii, tibialis anterior, left abductor digiti minimi, and left vastus lateralis muscles; whereas maximum voluntary contraction did not reveal abnormalities [Figure - 2]. Peripheral nerve conduction studies - including motor nerve conduction velocity and amplitude of the motor unit potential of the right median, ulnar (including axillar stimulation), peroneal, and left tibial nerve; and antidromic sensory nerve conduction velocity and amplitude of sensory nerve action potential of the right median and ulnar and both sural nerves; and F-wave latencies of the right median, ulnar, peroneal and left tibial nerve using surface electrodes - detected neither conduction block nor delay, and amplitudes of motor unit potentials were normal (>7 mV). Amplitudes of motor responses from both abductor digiti minimi and tibialis anterior muscles after cortical (>1.5 mV) and spinal (>10 mV) magnetic stimulation were normal, as were the latencies and the central motor conduction time. Visual and somatosensory evoked potentials showed normal responses in amplitudes and latencies. X-ray, computed tomography of the chest, and ultrasound of the thyroidal gland and abdomen were normal. The 9-hole-peg test showed reduced performance of the dominant hand (mean: dominant hand: 22.9 s, non-dominant hand 18,0 s), pressure of finger grip was 0.36 bar for the right and 0.42 bar for the left hand (mean). The paced auditory serial addition test (PASAT) revealed cognitive impairment (26 of 60 answers). Clinical, cMRI, EEG, electromyography and laboratory findings led to the diagnosis of Hashimoto′s encephalopathy associated with a lower motor neuron disease, and high-dose methylprednisolone was administered intravenously (1000 mg/d) on five following days. Then tapering of methylprednisolone was started at demission, followed by oral administration, 20 mg per day. The concomitant medication included riluzole for 3 years and esomeprazol, calcium, vitamin D3 and risedrone acid starting with the initiation of the steroid therapy. After 6 weeks, the patient presented with persistent dysarthria while he achieved gait stability, being able to play soccer, and fasciculations completely disappeared. Emotional instability and aggressive behavior were reduced significantly. TPO antibodies were decreased (385 U/ml). Control cMRI showed no alteration, especially no new lesions. Concentric needle myography again gave evidence of acute denervation, showing fibrillation potentials and positive sharp waves but no fasciculations in the right deltoideus, abductor digiti minimi, and vastus lateralis muscles, and in the left extensor digitorum communis and tibialis anterior muscles. Chronic denervation was found in the left extensor digitorum communis and tibialis anterior muscles. Further neurophysiological recordings, including peripheral nerve conduction studies, motor responses after cortical and spinal magnetic stimulation, visual and somatosensory evoked potentials, were normal again. Repetition of the 9-hole-peg test showed mild improvement of the dominant hand (mean: dominant hand: 21.9 s, non-dominant hand 19.1 s); pressure of finger grip was 0.41 bar for both hands (mean). The PASAT revealed persistent concentrative and cognitive deficits (28 of 60 answers). Overall, the tests showed slight improvement, and the patient underwent new intravenous administration of methylprednisolone. Discussion We here demonstrated a central nervous system disease as shown by the presence of attention deficit and cognitive deficit, and by magnetic resonance imaging revealing multiple small subcortical white matter lesions interpreted as Hashimoto′s encephalopathy by the presence of TPO antibodies. The presence of intrathecal antithyroid antibodies, as recently proposed to diagnose Hashimoto′s encephalopathy, was not tested.[8] The EEG alteration and slightly elevated CSF protein content may be additional features of HE, as these findings are present in 80-90% of HE patients, whereas diffuse subcortical MRI signal abnormalities may occur in HE or may be absent.[2],[3],[9],[10] In addition, we found clinical and electromyographic evidence for lower motor neuron disease. Contrary to this, in other cases of CNS disorder reported in the literature, the motor neuron affection was a peripheral nerve disorder (e.g. multifocal motor neuropathy).[5],[6],[7] The diagnosis of amyotrophic lateral sclerosis (ALS) was not made because the El Escorial criteria (1998) were not fulfilled as signs of both upper and lower motor neuron lesions in the same body region were not found by clinical and paraclinical means. As typical features like positive familiar history, gynecomastia, testicular atrophy, gigantism or hyperglycemia were absent, cognitive impairment was obvious, and cranial MRI was abnormal, Kennedy disease was not 6 considered. In addition, as clinical features like muscle cramps and stiffness, hyperhydrosis, and sensory symptoms were absent, symptoms did not fluctuate in severity over periods of months but were chronic progressive, bulbar signs were prominent in our patient and EMG did not reveal doublet or multiplet myokymoc discharges, this case did not fit into a phenotypic variant of autoimmune peripheral nerve hyperexcitability, which is considered to be located in the motor nerve terminal or intramuscular aborization and associated with immune disorders, i.e. the presence of serum voltage-gated potassium antibodies. This case may therefore also respond to the treatment with corticosteroids.[11]After repeated high-dose intravenous methylprednisolone administration followed by oral tapering, TPO antibodies decreased and central nervous system symptoms improved paralleled by an improvement of gait stability, remission of fasciculations confirmed by electromyographic recordings, and slight but not significant improvement of the motor function of the dominant hand. We have here, to the best of our knowledge, described the first case of parallel occurrence of CNS affection by Hashimoto′s encephalopathy and pure lower motor neuron disorder with unusually slow progression. Improvement of both cerebral and lower motor neuron symptoms was achieved by administration of glucocorticoids, suggesting a common pathogenetic mechanism for these clinically distinct diseases. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06097f2.jpg] [ni06097f1.jpg] |
| |||||||||

{kind=link}
{kind=link}