 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
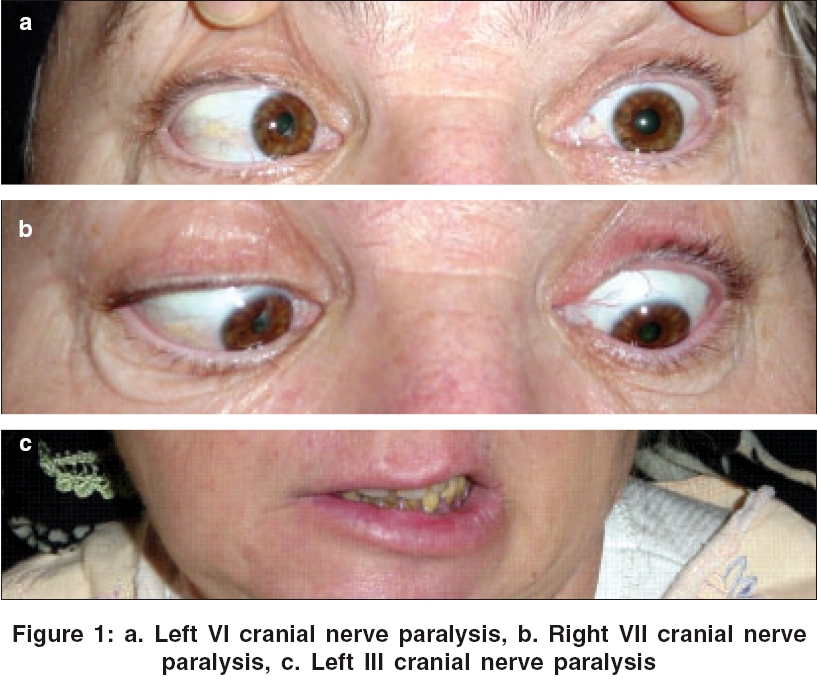
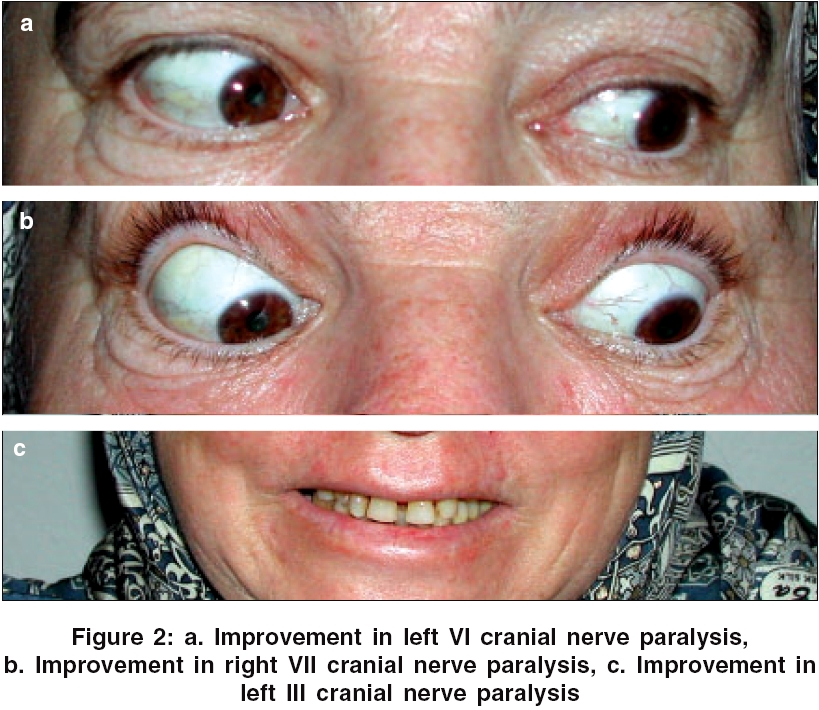
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 308-309 Case Report Simultaneous multiple cranial nerve neuropathies and intravenous immunoglobulin treatment in diabetes mellitus Uluduz Derya, Bozluolcay Melda, Ince Birsen, Kiziltan Meral Department of Neurology, Istanbul University Cerrahpasa Medical Faculty, Istanbul Date of Acceptance: 20-Aug-2006 Code Number: ni06100 Abstract Asymmetrical, simultaneous multiple cranial nerve palsies and mild signs of peripheral neuropathy in diabetic patients may cause difficulties in diagnosis as they are relatively rare. A case of a 55-year-old diabetic woman who developed simultaneous right VII and left III, IV, VI cranial nerve palsies with spared pupils is presented here. We also discuss the role of intravenous immunoglobulin (IVIG) in the management of this condition and suggest that simultaneous multiple cranial palsies may have a good response to IVIG treatment. Keywords: Diabetes mellitus, intravenous immunoglobulin; multiple cranial nerve palsies Introduction Simultaneous multiple cranial neuropathies are relatively rare, while isolated cranial nerve palsies are frequently encountered in patients with diabetes mellitus.[1],[2] The role of immunotherapy in this condition is also still debatable. This article presents a case with simultaneous multiple cranial nerve palsies and discusses the role of intravenous immunoglobulin (IVIG) treatment in the management of this condition. Case Report A 55-year old woman presented with a 2-week history of headache, blurred vision and diplopia. Her past medical history was unremarkable, except an uncontrolled type II diabetes mellitus for 12 years. Her neurologic examination revealed right peripheral facial paralysis, ptosis and restricted left eye movements in upward, downward, inward and outward directions with spared pupils [Figure - 1]. Funduscopic examination revealed signs of diabetic retinopathy. She was screened for metabolic, vascular, demyelinating, infectious, paraneoplastic, neoplastic and autoimmune neuromuscular junction diseases. In laboratory investigations, high lipid profiles and glucose levels were detected. Radiological findings, including cranial computed tomography (CT), magnetic resonance imaging (MRI), thorax and abdominal CT and vertebrobasillar system doppler ultrasonography, were normal. The nerve conduction studies indicated a mild polyneuropathy. Facial nerve electroneurography revealed 65% fiber loss in the right facial nerve. Electrically evoked blink reflex (BR) was absent in the same side. BAEP examination showed an increase in the fifth wave latency and EMG was normal for neuromuscular junction disease. Apart from the nonsteroidal anti-inflammatory medication (Diclofenac sodium 150 mg/day), she was put on insulin treatment as well. There was no change in glucose levels even though the dose of insulin was gradually increased to 58 units/day and her complaints were persisting. IVIG treatment was initiated on the 15th day of her hospitalization with a dose of 0.4g/kg/day and this treatment was continued for 5 days. On the 1st day of this treatment, an obvious decrease in blood glucose level was observed. During the first week, the right peripheral seventh nerve palsy was partially recovered and electrophysiological BR reflex was obtained. All defective cranial nerve findings disappeared during the first month and did not clinically recur during the following 8 months [Figure - 2]. Discussion Although proximal neuropathies are common entities in diabetic patients, simultaneous multiple cranial neuropathies are relatively rare.[2],[3] There have been no decisive and clear evidences concerning the development mechanisms of poly-cranial neuropathies. The clinical absence of radiological and laboratory findings that might point to the localization of the disease brings to mind an inflammatory process. There is increasing evidence that the characteristic lesion in proximal diabetic neuropathy is inflammatory (immune) vasculitis that induces ischemic nerve fiber degeneration.[3] All investigations, with the exception of biopsy, have been carried out in our case and we also think that the immune mechanism has a relative role in the pathogenesis. The patient might have autoimmune neuromuscular junction disease, but we ruled it out based on the involvement of the seventh cranial peripheral nerve, the latency in eye-blinking response and the negative result in myasthenic test determined by EMG analysis. Immunotherapy, including IVIG, was reported to be effective in few patients with diabetic neuropathy, like radiculoplexopathy, etc.[4] The action mechanism of IVIG in autoimmune disorders is still uncertain. Various proposed mechanisms include the neutralization of the pathogenic antibodies by anti-idiotype antibodies, the attenuation of complement-mediated tissue damage and the saturation or functional blockage of Fc receptors on demyelinating macrophages.[5] Although it is not possible to reach a decisive conclusion about the action mechanism in our patient, the high glucose level was reduced after the first day of IVIG treatment and clinical recovery began on the second day. The clinical symptoms had totally disappeared at the end of the first month. There was no recurrence of these symptoms within the next 8 months following treatment The observations made with this patient suggest that immunoglobulin may play a role in the management of this particular medical condition. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06100f2.jpg] [ni06100f1.jpg] |
| |||||||||

{kind=link}
{kind=link}