 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 310-311 Brief Report Analysis of dystrophin gene deletions by multiplex PCR in eastern India Basak Jayasri, Dasgupta UmaB, Banerjee TapasK, Senapati AsitK, Das ShyamalK, Mukherjee SubhashC Department of Biophysics, Molecular Biology and Genetics, University of Calcutta, 92, A.P.C. Road, Kolkata Date of Acceptance: 04-Aug-2006 Code Number: ni06101
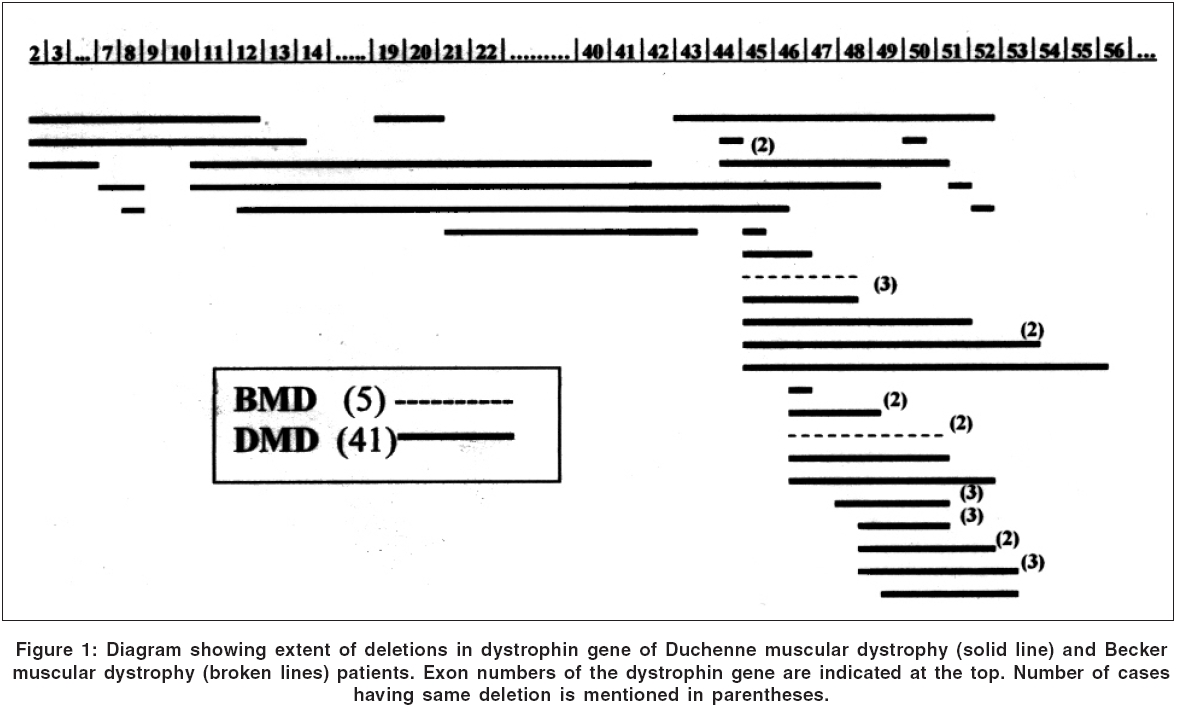
The most common genetic neuromuscular disease of childhood, Duchenne and Becker muscular dystrophy (DMD/BMD) is caused by deletion, duplication or point mutation of the dystrophin gene located at Xp 21.2. In the present study DNA from seventy unrelated patients clinically diagnosed as having DMD/BMD referred from different parts of West Bengal, a few other states and Bangladesh are analyzed using the multiplex polymerase chain reaction (m-PCR) to screen for exon deletions and its distribution within the dystrophin gene. Out of seventy patients forty six (63%) showed large intragenic deletion in the dystrophin gene. About 79% of these deletions are located in the hot spot region i.e., between exon 42 to 53. This is the first report of frequency and distribution of deletion in dystrophin gene in eastern Indian DMD/BMD population. Keywords: BMD, deletion, DMD, dystrophin gene, muscular dystrophy Introduction Dystrophin gene located at Xp 21.2 is the largest known gene with 79 exons and produces a 427 kd protein involved in the contractile apparatus of the muscle cells. Inactivation of the gene by deletion /duplication of one or more exons or point mutation produces the X-linked recessive disorders Duchenne and Becker muscular dystrophies. Frequent occurrence of Alu repeats make intragenic deletion the most common genetic lesion accounting for two third of the cases of DMD and BMD combined incidence of which is 33 in 1,00,000 male birth. Proportion and patterns of deletions in the dystrophin gene prevalent among the DMD/BMD patients in eastern India detected by multiplex PCR (m-PCR) is reported in the present work.Materials and Methods Patients and samples Clinical diagnosis was based on physical examination, progressive muscle weakness, muscle strength, high level of serum CPK, calf hypertrophy, positive Gower′s sign, positive Pradhan′s sign and myopathic changes on electromyelography (EMG). Blood samples were collected from clinically diagnosed DMD and BMD patients, attending the clinics of Bangur Institute of Neurology, Kolkata; Neurology Department of Medical College and Hospital, Kolkata; Neurology Department of Peerless Hospital, Kolkata and Hospitals of Bangladesh. Ages ranged from one year to sixteen years with median at 5 years. Six patients were from Bangladesh, one from Bihar, ten from Kolkata, nine from Hoogly, six from south 24 parganas and the rest are from different parts of West Bengal. Written informed consent was obtained from all participants before drawing their blood. Deletion screening by multiplex PCR (m-PCR) DNA was isolated from 5-6 ml of EDTA-blood following the standard procedure.[1] Detection of intragenic deletion by m-PCR was standardized following the methods described earlier[2],[3] and using primer sets purchased from Sigma Chemicals (USA). Amplification was performed for 25 cycles on an Applied Biosystem automatic thermocycler. PCR product was resolved by electrophoresis in 2% agarose gel and visualized on UV-transilluminator after ethidium bromide staining. Results and Discussion Out of seventy unrelated patients of DMD (58) and BMD (12), forty five (64%) were from Hindu community and twenty five (36%) were from Muslim community. Detailed family history was available in forty-five families and there was no previous history of the disease in twenty-eight (62%) families. All the patients had pseudohypertrophy of calf muscle and weakness of proximal muscles of lower limbs. The highest and lowest serum CPK values among these seventy patients are recorded as 35200 IU/l and 195 IU/l respectively, both observed in DMD patients. Out of seventy patients tested, forty-six showed intragenic deletion in the dystrophin gene. The percentage of cases having gene deletions in eastern India is 65.7%, which is slightly lower than that reported in the north India.[4] There are thirty eight deletions (82.61 %) located in the hot spot region (between exon 42 to 53), five (10.87 %) deletions at the proximal hot spot (exon 1 to 20) and only three (6.52 %) between exon 21 to 42. Largest deletions found were in three DMD patients ranging i) exon 12 to 45, ii) exon 11 to 48 and iii) exon 11 to 41 spreading in both the hot spot regions. Their ages of onset are 5, 4, 3 years respectively. Pattern of deletions is depicted in [Figure - 1]. Distribution of deletion in the dystrophin gene is known to vary from population to population. For example, percentage of deletion in the central hot spot region in Chinese is approximately 50% of all deletions,[4] whereas in north India[4] it is around 80%, with which our data conforms. Racial differences in incidence rate of DMD have been suggested.[5] We have observed a higher incidence of cases in Muslims. However the data is not large enough to be statistically significant. Molecular detection of dystrophin gene mutation is essential for carrier detection and genetic counseling. This work would help to achieve the goal in eastern region. Acknowledgements Financial support from DST, GOI, (SR/WOS-A/LS-1071/2003) is acknowledged. Advice from Professor B. Mittal is gratefully acknowledged. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06101f1.jpg] |
| |||||||||

{kind=link}