 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
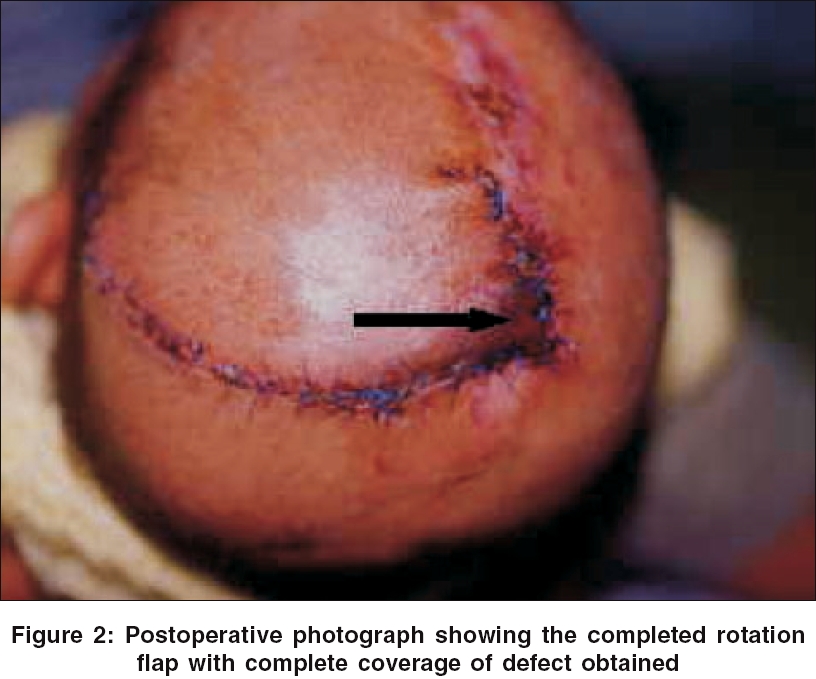
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 312-313 Brief Report Aplasia cutis congenita of the scalp: Therapeutic modalities Shivakumar SK, Dwarakanath S, Swaroop Gopal, Venkataramana NK Department of Neurosurgery, Manipal Institute for Neurological Disorders, Bangalore - 560 017, Karnataka Date of Acceptance: 22-Feb-2006 Code Number: ni06102 Abstract Agenesis of scalp is an uncommon but well-recognized clinical entity. Congenital scalp and skull defects can be either obvious or occult; over 300 cases have been reported in literature. Aplasia cutis congenita (ACC) is recognized as a heterogeneous disorder, all characterized by focal absence of the epidermis, dermis and sometimes the calvarium and/or dura. We present a case of ACC in an infant whose mother was exposed to a teratogenic drug (Methimazole - an antithyroid drug) during pregnancy. This case report is presented to highlight the steps to successful management. Definitive full thickness scalp cover at the earliest avoids secondary infection, eschar formation and exsanguination. Keywords: Aplasia cutis congenital, management, teratogenic Introduction Aplasia cutis congenita (ACC) is a heterogeneous disorder, all characterized by focal absence of the scalp and sometimes the calvarium and/or dura. We present a case of ACC whose mother was exposed to a teratogenic drug during pregnancy and review the relevant literatureCase Report A male child born at term was noticed at birth to have multiple scalp defects along the midline. He was born of a non-consanguineous marriage and there was no family history of congenital anomalies. The mother was on tablet Methimazole for thyrotoxicosis. Initially, regular dressings were performed. However, the scalp defects did not heal completely. The infant was referred to us when he was 3 months old. There were three lesions over midline scalp arranged in a linear fashion [Figure - 1]. The frontal lesion was the smallest, measuring about 1.2 cm in diameter. The second (posterior-frontal) was 3 x 2.5 cm in size, while the parietal was 4 x 3.5 cm in size [Figure - 1]. All the lesions were covered by a densely adherent thick black eschar. Neurologically, the child had no other obvious neurological deficits. He had short stubby toes in both the feet but no X-ray defects. The child was advised to continue dressing with Bacitracin ointment as review of literature revealed povidone iodine to be a desiccating agent and not recommended for usage in ACC. The anterior-most lesion healed completely over a period of 4 weeks. The posterior two lesions did not heal despite repeated dressings and there were several episodes of fresh bleeding from the lesions. The last episode of bleeding from the scalp defect was fairly severe and necessitated admission for definitive surgery. A thorough saline-wash was performed and the eschars were gently separated. A full thickness pedicle rotation flap from the adjacent scalp was performed [Figure - 2]. The wound healed well over the following 2 weeks without residual defects. Discussion ACC is a skin defect of multivariate etiology occurring at birth. Typically, the lesions appear as small ulcerations that usually heal spontaneously. Larger lesions may be associated with underlying bony lesions and can cause death secondary to infection or hemorrhage, especially if from the venous sinuses. In the past, birth trauma, congenital syphilis or skin avulsion by attached amniotic bands was considered a causative factor.[1],[2]First described in 1826, Frieden classified ACC based on etiology and manifestation into nine groups.[3] Approximately 25% of the reported cases are familial, a vast majority (69%) showing an autosomal dominant inheritance. Our case fits into group 8, which is caused by viral infections and specific teratogens (e.g., Methimazole).[4],[5] Eighty-four percent cases of ACC involve the scalp, of which 75% are single. Most are situated in the midline. Extension through dermis, galea and bony calvarium occur in 35% of cases. When left untreated, these defects desiccate and form an eschar. As this dries, their edges retract, placing tension on the underlying dura. Frequent dressings tend to pull the eschar and cause frequent bleeds. If a tear occurs over the sagittal sinus, a life-threatening hemorrhage can result. The site often becomes secondarily infected. If there is a dural tear and the subarachnoid space is exposed, meningitis can result. Management strategies are based on the size and presence of an underlying skull defect. Smaller eschars with intact calvarium can be allowed to heal spontaneously with routine wound care. Large lesions with an underlying skull defect require surgical closure to prevent massive hemorrhage. When primary closure is not possible, a full thickness vascularized pedicle graft can be utilized. Genetic counseling is useful when ACC is inherited. Systemic examination is necessary to rule out any other defects.[1],[5] References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06102f1.jpg] [ni06102f2.jpg] |
| |||||||||

{kind=link}
{kind=link}