 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
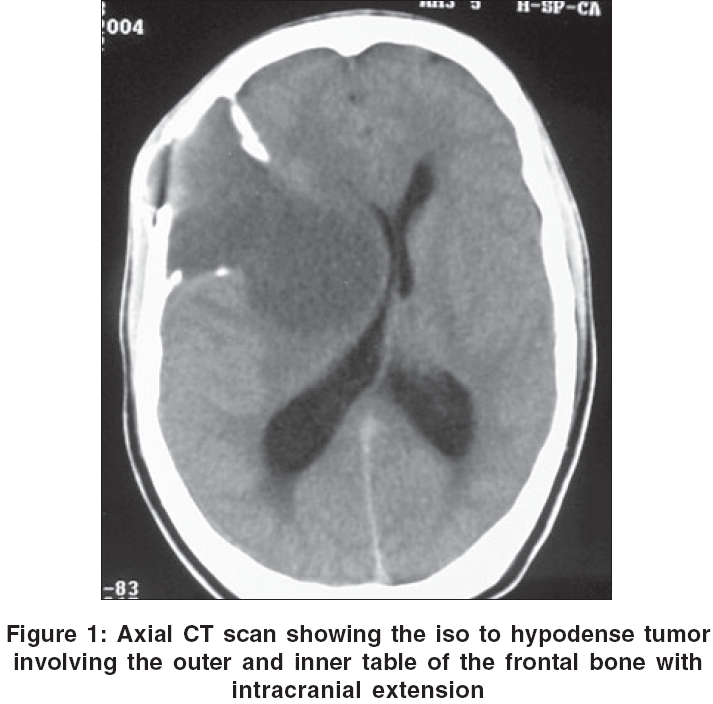
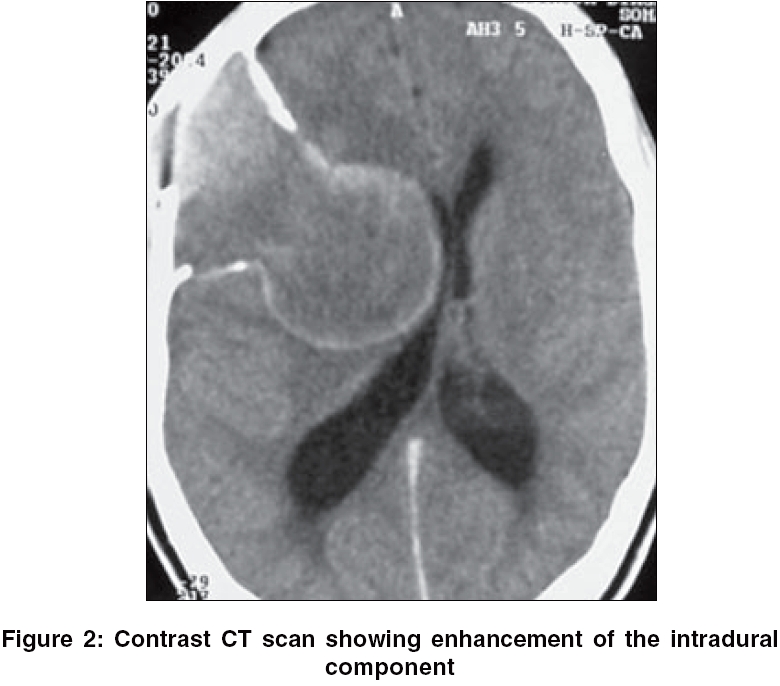
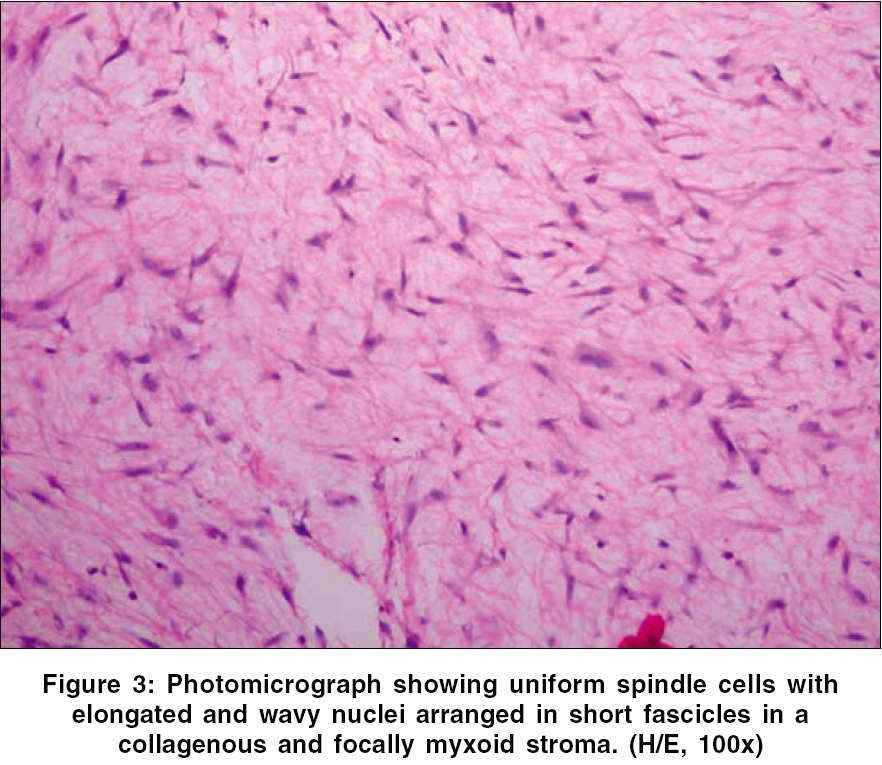
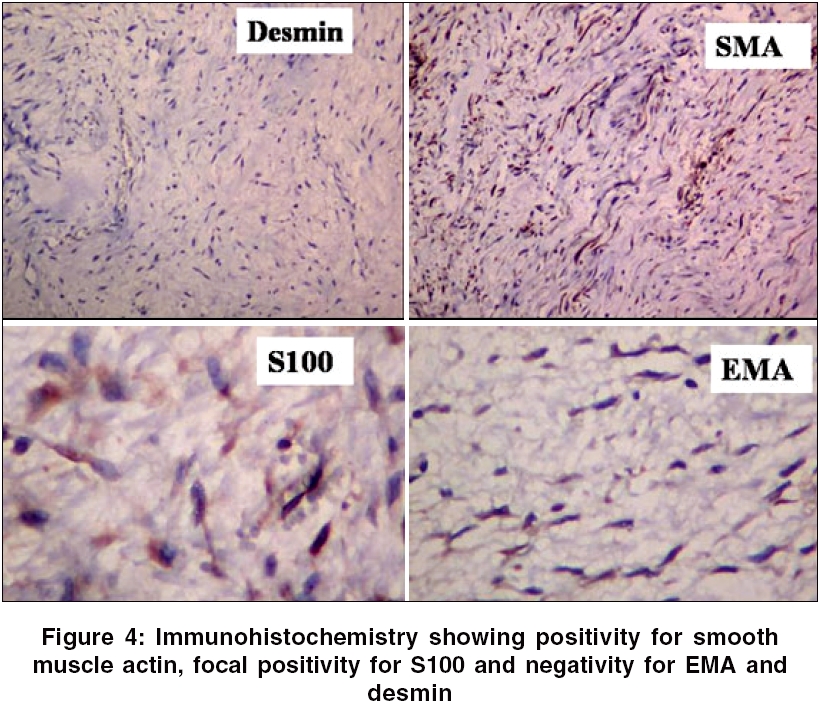
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 314-315 Brief Report Desmoplastic fibroma of the frontal bone Lath Rahul, Ranjan Alok, Ratnam BG, Gowrishankar Swarnalata Department of Neurosurgery, Apollo Hospitals, Hyderabad - 500 033, Andhra Pradesh Date of Acceptance: 20-Feb-2006 Code Number: ni06103 Abstract Desmoplastic fibroma is a benign but locally aggressive tumor arising usually from the mandible, pelvis and long bones with a potential for recurrence. We report a case of desmoplastic fibroma of the frontal bone in a young male. Keywords: Desmoplastic fibroma, skull Introduction Desmoplastic fibroma is a rare benign but locally aggressive tumor, arising predominantly in the mandible, pelvis and long bones.[1] Only about 10 cases have been reported. We report the first case from India.Case Report An 18-year-old male presented with headaches and a scalp swelling of 1 month duration. On examination there were soft right-sided pyramidal signs. There was a bony swelling in the left frontal region. CT scan [Figure - 1] showed a mass involving the left frontal bone with intracranial extension. There was an isodense intradural component which enhanced with contrast [Figure - 2]. He underwent a craniotomy and total excision of the tumor. Per-operatively the tumor was found to arise from the bone and had broken through into the scalp. Part of the tumor was extradural and there was a large well-defined intradural component extending upto the lateral ventricle. Tumor was excised radically together with involved bone and the dura. Duroplasty was done. Histopathology revealed that the tumor was composed of uniform spindle cells with elongated and wavy nuclei arranged in short fascicles with the stroma being collagenous and focally myxoid [Figure - 3]. There was absence of nuclear pleomorphism, mitosis and necrosis. The architectural pattern typical of a fibroblastic meningioma was absent. Immunohistochemistry showed that the cells were positive for smooth muscle actin, vimentin and focally positive for S-100 protein [Figure - 4]. Epithelial membrane antigen (EMA), desmin, estrogen and progesterone receptors were negative. The features were thus in favor of a desmoplastic fibroma of the bone. The patient is asymptomatic at one-year follow-up.Discussion Desmoplastic fibroma accounts for 0.3% of all benign bone tumors.[1] The common sites of occurrence are mandible, pelvis and long bones.[1] Rarely the tumor occurs in the skull bones.[2],[3],[4],[5],[6] Majority have occurred in female adult patients, while one case of congenital desmoplastic fibroma was reported in a male child.[3] The duration of symptoms ranged from 1 month to 12 years and the age group ranged from 3 months to 86 years. The clinical presentation included headache, cranial asymmetry, ear symptoms and skull mass. The tumors reported so far have involved the diploe, inner and outer tables of the skull. In one case there was extensive involvement of the dura.[6] In no case was brain invasion reported. Our case had a large intradural component, indicative of local aggressiveness of this tumor. Radiographic findings are non-specific and final diagnosis depends upon histology. Skull X-rays revealed lytic lesions without sclerosis.[3],[4] CT scans show hypodense lesions involving both the tables of the skull with bone fragments and soft tissue component.[5],[6] On MRI, the lesion is iso-intense on T1-weighted images, iso to hyperintense on T2-weighted images with gadolinium enhancement.[6] The differential diagnosis for smaller lesions presenting as lytic skull lesions, include simple bone cyst, aneurysmal bone cyst, eosinophilic granuloma and giant cell tumor.[6] The radiological differential diagnosis of large cranial vault lesion with dural and intracranial involvement, like in our patient, include invasive meningiomas, hemangiopericytomas and metastases.[6] Desmoplastic fibroma histologically and biologically resembles a desmoid soft tissue tumor.[1],[6] It is composed of slender or plump fibroblasts with ovoid nuclei dispersed within a collagenous and myxoid matrix.[1],[4],[6] Lack of mitotic figures, hypercellularity and pleomorphism help to distinguish this tumor from malignant tumors like fibrosarcoma. Another important feature of this tumor is the absence of osteoid tissue formation.[4] Fragments of mature bone may be seen within the lesion but new bone formation is lacking, which distinguishes it from fibrous dysplasia. The lesions which come in the histological differential diagnosis include fibrous dysplasia, fibrosarcoma, malignant fibrous histiocytoma and non ossifying fibroma.[6] Immunohistochemistry may show positivity for smooth muscle actin, desmin, muscle-specific actin and vimentin.[1],[6] Immunohistochemistry for cytokeratin, EMA, S-100 and CD68 is negative.[6] In our patient S-100 was focally positive in less than 25% of the spindle cells and the significance is unclear. On electron microscopy the predominant cell component appears to be myofibroblasts.[1] This along with positivity for smooth muscle actin would point towards a myofibroblastic origin of this tumor. Surgery followed by cranioplasty is the treatment of choice for desmoplastic fibroma of the skull bones. Most reported cases have been treated with complete excision of the lesion.[2],[3],[4],[5],[6] In cases of dural involvement, like in our case, excision of the dura followed by duroplasty is mandatory. There are no reports of recurrence or metastases arising from the skull lesions. The unusual features in our case were the occurrence of this tumor in a male patient and the presence of dural invasion with a large intradural component which has not been previously reported. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06103f4.jpg] [ni06103f3.jpg] [ni06103f1.jpg] [ni06103f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}