 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
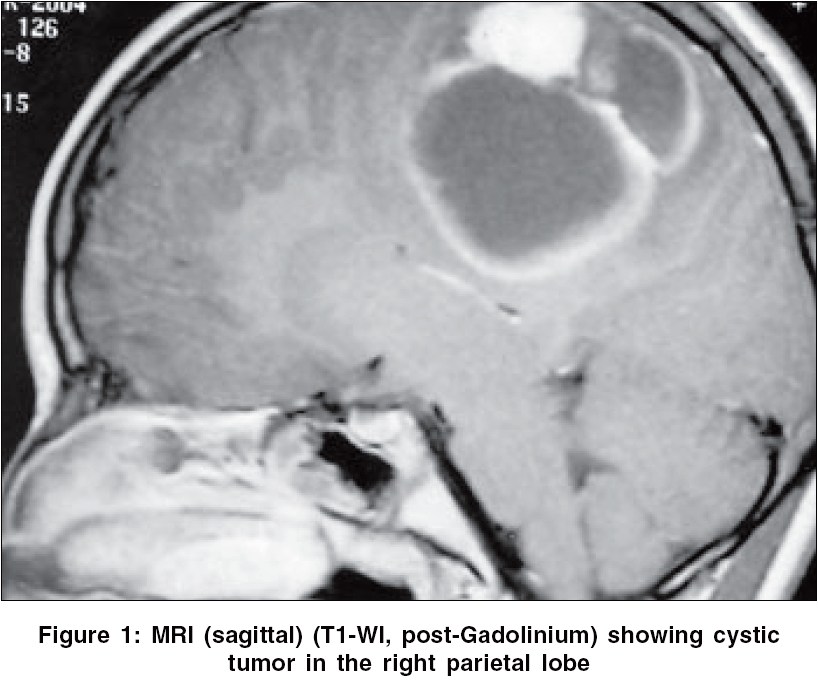
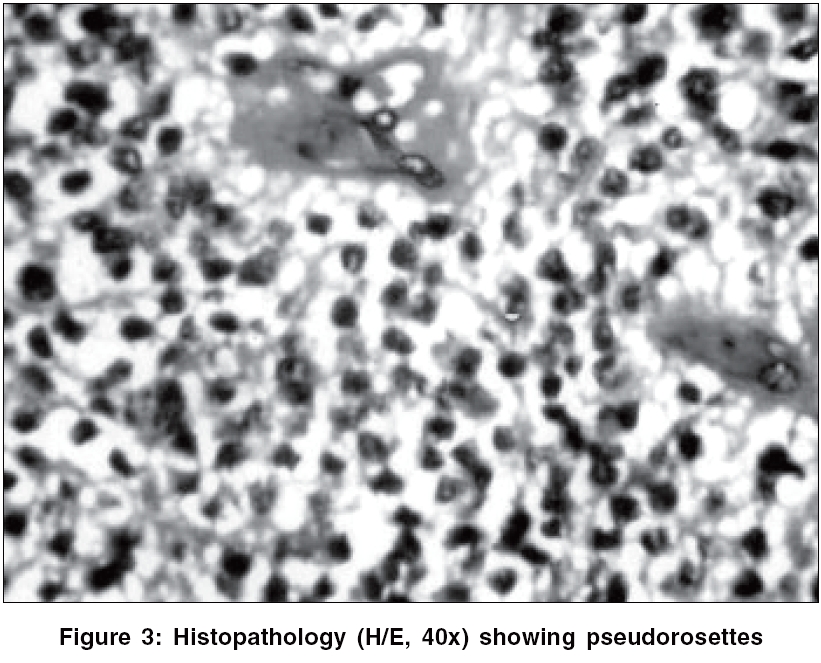
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 321-322 Letter To Editor Brain surface ependymoma in a child Bhatoe HarjinderS, Dutta Vibha Departments of Neurosurgery and Pathology, Army Hospital (Research and Referral), Delhi Cantt, New Delhi Date of Acceptance: 30-Mar-2006 Code Number: ni06111 Sir, Ependymoma is a slow growing glial tumor originating from the ventricular lining or central canal and is composed of neoplastic ependymal cells. Usual site of these tumors in children is the posterior fossa. Exceptionally, they may occur supratentorially, without any connection to the ventricular lining. We report one such tumor in a child, diagnosed as a clear cell ependymoma. An 11-year-old girl was admitted with a 2-months history of intermittent bouts of generalized headache, often accompanied by vomiting. There was no history of seizures, alteration in sensorium, ataxia or any limb weakness. Clinical evaluation except for bilateral papilledema was unremarkable. MRI brain (T1- and T2-weighted and T1-gadolinium sequences) showed low-intensity intraaxial tumor in right parietal lobe, reaching the surface, on T1-WI with peripheral enhancement with intravenous Gadolinium. The contents had bright signal intensity on T2-WI. A solid contrast-enhancing portion was seen over the medial aspect of the tumor [Figure - 1][Figure - 2]. There was no edema of the brain. Craniotomy revealed cortical and subcortical cystic tumor, containing a straw-colored fluid that could be separated from the surrounding brain without any difficulty. No connection to the ventricular wall was seen. Tumor was totally excised. Postoperative period was uneventful. Histopathology revealed a highly cellular tumor with a sharp tumor-parenchymal surface. The tumor cells had a clear perinuclear halo and were seen to lie within a fibrillary background. Perivascular pseudorosettes were obvious in most of the sections [Figure - 3]. No mitotic figures were identified. Immunohistochemistry revealed positivity for GFAP, S-100 and vimentin and negativity for synaptophysin. Based on these features, a diagnosis of clear cell ependymoma (WHO grade II) was made. At present, she is on follow-up and CT after 2 years has not revealed any recurrence. Rarely, supratentorial ependymomas may occur outside the ventricular system, particularly in children. It is likely that in such a situation, they arise from ependymal cell rests (embryonic ependymal remnants) in brain parenchyma.[1] Supratentorial tumors often exhibit cystic components and extensive calcification may be observed.[2] Microscopically, diagnostic features are perivascular pseudorosettes and ependymal rosettes. Mitotic figures are rare. The cells display a clear perinuclear halo akin to oligodendroglia and the tumor can mimic oligodendroglioma, central neurocytoma and clear cell renal carcinoma. Although clear cells resembling oligodendrocytes are known to occur in ependymomas,[1] tumors composed primarily of such cells are rare. Clear cell ependymomas (CCEs) are well delineated tumors characterized by sharp circumscription, hypervascularity as reflected by contrast enhancement on CT and MRI. These tumors have a predilection for supratentorial region in children; nine of the 10 children with CCEs reported by Fouladi et al had supratentorial tumors. Histologically, CCEs show reactivity to GFAP, S-100 and vimentin. Moreover, ependymomas lack synaptophysin reactivity, which is seen more often in central neurocytoma. Electron microscopy shows complex intercellular junctions, surface microvilli and microrosette formation, thus underscoring the importance of EM in diagnosis. Unlike the central neurocytomas and glioneurocytomas, CCEs lack secretory granules, vesicles and synapses. While the issue of radiotherapy in ependymomas in children is still not completely settled, it is generally advised to give radiotherapy even after complete removal.[3] Without radiotherapy, these tumors can have early recurrence and extraneural metastases.[4] Roncaroli et al[5] recently reported three cases of brain surface ependymoma, one of whom was in a child. No radiation therapy was given and the outcome was correlated to the completeness of excision and the tumor grade. There is no known prognostic significance attached to clear-cell change in ependymomas.[6] CCEs are unusual variants of ependymomas. Ependymomas occurring supratentorially without any connection to the ventricular system are rare. The tumors are slow growing, cystic and can be completely excised. Histopathological appearances are typical and the diagnosis can be further confirmed by immunohistochemistry. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06111f1.jpg] [ni06111f3.jpg] [ni06111f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}