 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
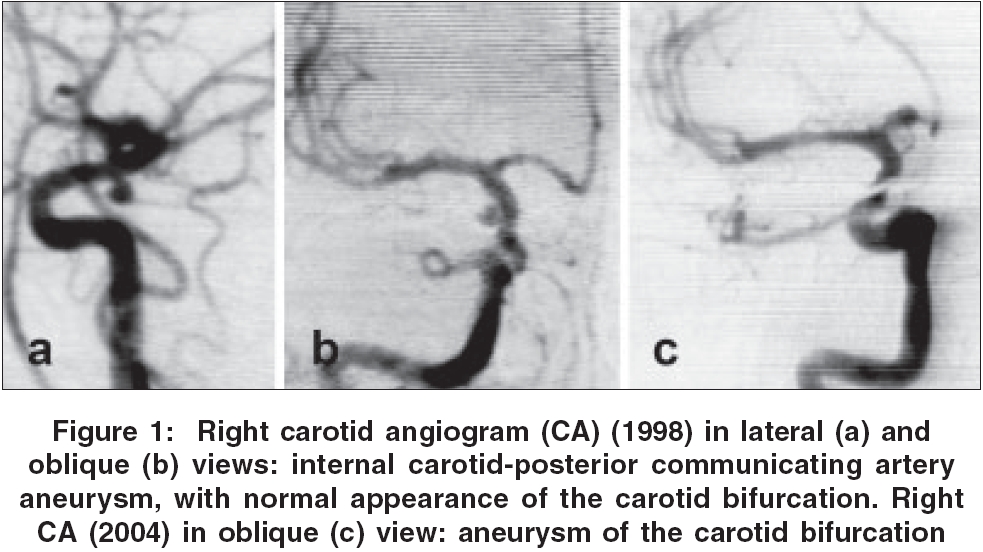
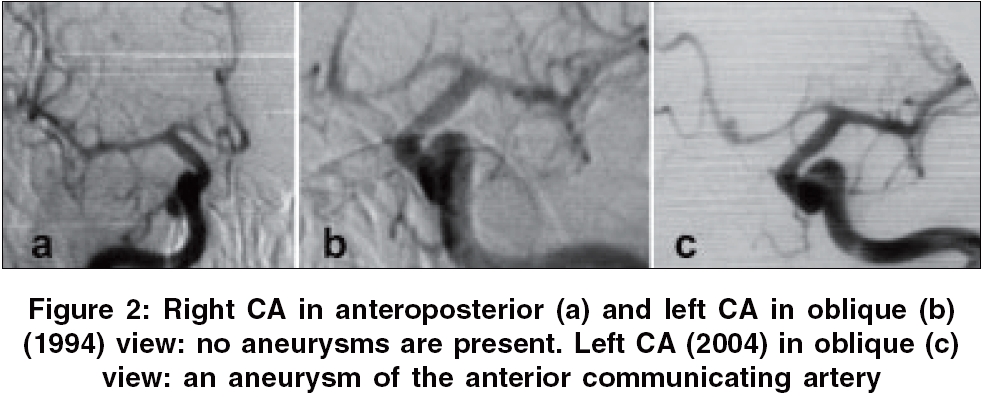
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 324-325 Letter To Editor De novo formation and rupture of an intracranial aneurysm Danilo RadulovicV, Branislav Nestorovic D, Ljiljana Vujotic B, Vladimir Bascarevic L J Department and Institution, Institute for Neurosurgery,Clinical Center Serbia, Belgrade Date of Acceptance: 02-Aug-2006 Code Number: ni06113 Sir, De novo aneurysm is a newly formed aneurysm developing from a cerebral vessel which had appeared to be normal in a previous angiographic study. They have been usually discovered some time after successful treatment of aneurysms located elsewhere or after subarachnoid hemorrhage (SAH) of unknown origin.[1],[2],[3],[4],[5] This report concerns two such patients. Patient 1 A 40-year-old male, a chronic heavy smoker with uncontrolled hypertension, was admitted after SAH in grade II according to Hunt and Hess (H and H) scale. CT scan showed SAH predominantly located in the right Sylvian fissure. Four-vessel angiography demonstrated right internal carotid artery aneurysm [Figure - 1]a and b, in the region of the posterior communicating artery and no other aneurysms. The aneurysm was successfully clipped. Inspection of the carotid artery revealed no other abnormalities. The patient recovered completely, but later suffered from arterial hypertension and was treated with antihypertensive medication. The patient was readmitted five years later with new episode of SAH in H and H grade III. A CT scan revealed blood collection in the right Sylvian and insular cisterns. Four-vessel angiography demonstrated an aneurysm of the right internal carotid artery bifurcation [Figure - 1]c which was clipped with good postoperative course. Patient 2 A 41-year-old man, non-smoker with a history of arterial hypertension, was admitted after SAH in H&H grade II. CT scan revealed a SAH into basal cisterns and the interhemispheric fissure. Four-vessel angiography did not show any abnormalities or signs of spasm [Figure - 2]a and b. The patient refused control angiography and was lost to further follow-up. Ten years later, he was readmitted with a new episode of SAH in H&H grade III. CT scan showed a SAH and an intracerebral hematoma in the left frontal lobe. Angiography revealed an aneurysm of the anterior communicating artery [Figure - 2]c, which projected superiorly and filled by the left carotid artery. The aneurysm was clipped. Postoperatively the patient had slight dysphasia and disorientation, which gradually resolved. Crucial problem concerning de novo aneurysms is that what we assumed to be newly developed aneurysm may have been present already, but unrecognized at the time of the first angiography. We believe that none of our two de novo aneurysms were present in initial angiograms. In our first patient not only the angiograms, but surgical exploration also confirmed the absence of any lesion at carotid artery bifurcation. In our second patient, bilateral carotid and vertebral angiography covering multiple directional views and very long time interval between first and second SAH make false negative results very unlikely. Our observations and similar reports from literature demonstrate that de novo aneurysms can develop over some periods of time after initial SAH. Although there are no guidelines at present, periodic follow-up to detect de novo aneurysms is recommended by most authors,[1],[3],[4],[5] particularly in young patients with risk factors such as arterial hypertension,[2] smoking,[2],[4] multiple and familial aneurysms,[1] and congenital connective tissue disorders.[3] MR angiography and 3-dimensional CT angiography can be used as a good screening tool for de novo aneurysms. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06113f2.jpg] [ni06113f1.jpg] |
| |||||||||

{kind=link}
{kind=link}