 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
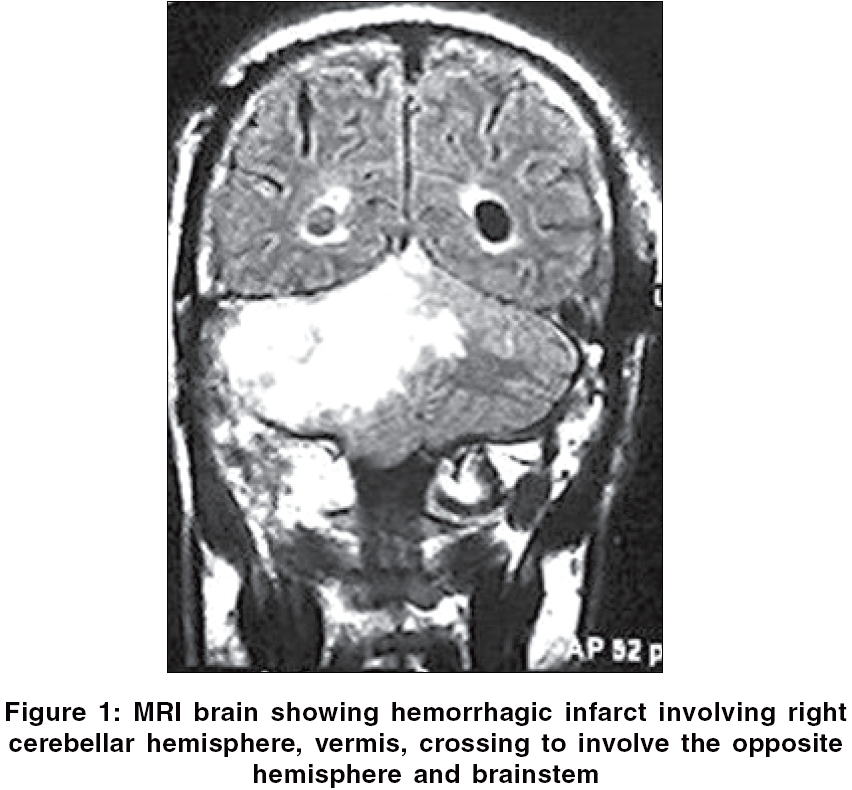
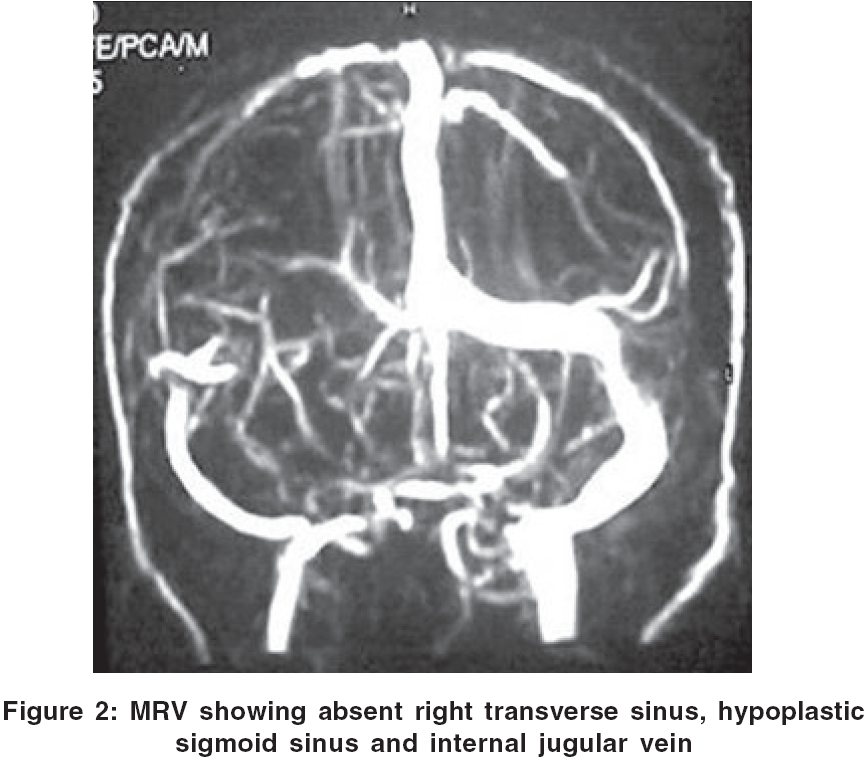
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 325-326 Letter To Editor Brain stem infarction: A complication of microvascular decompression for trigeminal neuralgia Singh Daljit, Jagetia Anita, Sinha Sanjiv Department of Neurosurgery, G. B. Pant Hospital, Delhi, J-71, Vijaylakshmi Apartments, Patparganj, Delhi Date of Acceptance: 01-Feb-2006 Code Number: ni06114 Sir, Microvasular decompression (MVD) of trigeminal nerve (TN) is the treatment of choice for typical trigeminal neuralgia in patients refractory to medical therapy. In experienced hands, this procedure is safe; however, the complication rate reported in different series is 1-4% with a mortality of 0.5%. The incidence of complications such as cerebellar and brainstem venous infarct, transverse sinus thrombosis following MVD is not known except for scanty case reports.[1] We encountered a rare complication of MVD for trigeminal neuralgia in a 54-year-old man. He presented with the right-sided facial pain in V2, V3 distribution, typical of trigeminal neuralgia, for a period of 6 years. He was refractory to medical treatment. MRI of brain was normal. Microvascular decompression of TN was done in semi-sitting position. Trigeminal nerve was compressed by superior cerebellar artery along the anteroinferior aspect. Superior petrosal vein got avulsed during retraction and hence was coagulated. A PTFE (polytetrafluro ethylene) patch was placed between TN and the superior cerebellar artery. Postoperatively, patient was conscious but response to command was delayed. On the first postoperative day, he became tachypnoeic, confused, dysarthric and ataxic with right-sided lower cranial nerve paresis and cerebellar signs. CT brain showed right cerebellar hemispheric hypodensity with hydrocephalus. Right VP shunt was done. CSF pressure was raised and CSF examination was normal. Postoperative MRI was suggestive of cerebellar and brain stem venous infarct. MR venogram revealed agenesis of right transverse sinus, hypoplastic right sigmoid sinus and internal jugular vein [Figure - 1][Figure - 2]. On the third postoperative day, the patient was intubated as he developed respiratory difficulty. Thereafter, he was managed conservatively as relatives did not consent for decompression of posterior fossa. Patient did not show improvement and died on the fifth postoperative day. Superior petrosal vein is an important draining vein of the posterior fossa. It is a constant vein and drains a very large area, including the anterior parts of cerebellum, posterior part of medulla and mesencephalon, anterior part of the pons and medulla. The coagulation of this vein during surgery may result into venous infarct in the mentioned territory.[2] However, the collateral veins take over the function of the coagulated vein and this is possibly the reason that in many patients operated for CP angle mass, surgery is uneventful even if this vein is coagulated. It is difficult to assess the functional capacity of the collateral venous channels and the neurological outcome depends upon the extent and the speed at which they develop.[3] In transverse sinus thrombosis, the proximal portion of transverse sinus is visible, but the distal portion of the transverse sinus, sigmoid sinus and jugular vein is not visible.[4] Contrary to the findings in transverse sinus thrombosis, in our patient, transverse sinus was not visible along its entire course and the sigmoid sinus and jugular veins were visible, supporting the diagnosis of transverse sinus hypoplasia or agenesis. This patient developed infarct, perhaps because of transverse sinus agenesis and inappropriate function of the collaterals. This case supports the fact that no vein should be coagulated, however small, but there is no alternative other than this when it gets avulsed during surgery. To avoid such a complication, the simplest and economical investigation is plain skiagram of skull to look for associated lateral sinus anomalies as the incidence of transverse sinus anomalies is 5-6%. It is dominant on the right side in approximately 43%, left side in 19% and equal in 37% of cases.[5] Plain skiagram of skull will reveal gross difference in the diameter of the two sides of jugular foramen. MR venogram can also be a useful investigation in preoperative work-up to exclude the dural sinus anomaly. References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06114f1.jpg] [ni06114f2.jpg] |
| |||||||||

{kind=link}
{kind=link}