 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
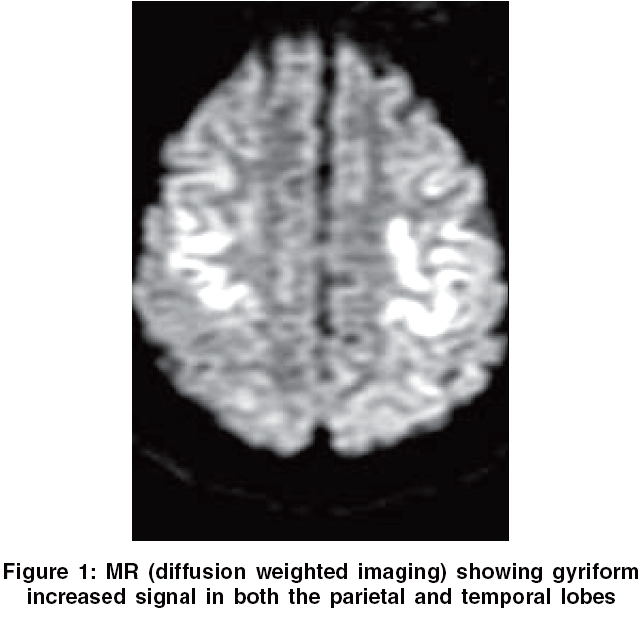
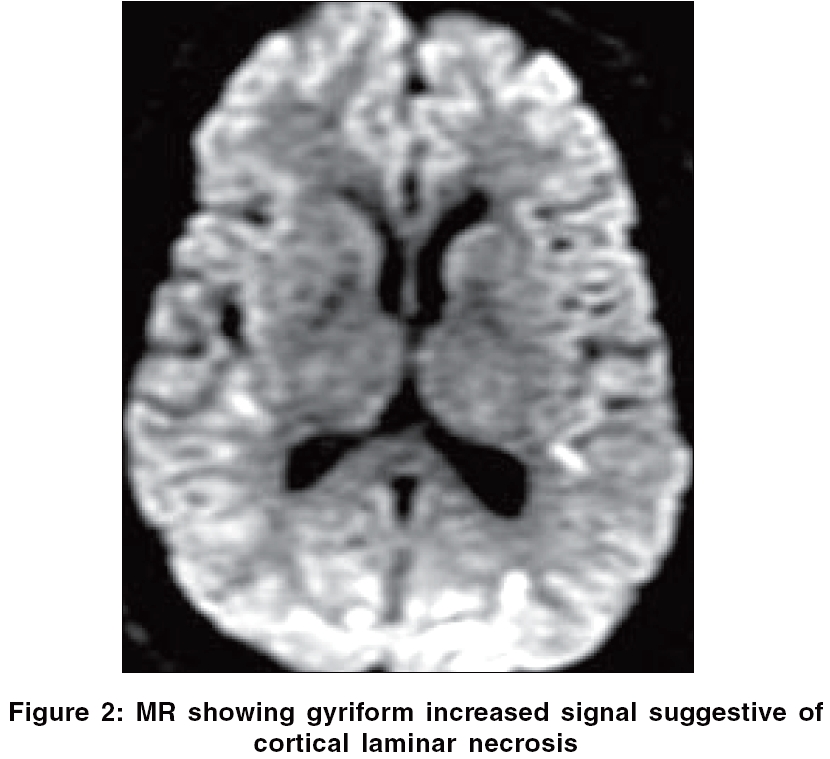
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 327 Neuroimage Cortical laminar necrosis following anoxic encephalopathy Sethi NK, Torgovnick J, Macaluso C, Arsura E Department of Neurology, Saint Vincent's Hospital and Medical Centers, New York Date of Acceptance: 05-Aug-2006 Code Number: ni06115 Neurology consultation was requested for status epilepticus on a 48-year-old male in the medical intensive care unit. Patient had been found unresponsive outside a bar by the emergency medical services. An empty bottle of bupropion was found on his person. Cardiopulmonary resuscitation had been initiated in the field and a peripheral pulse was detected after 10 min. Admission EtOH level was 175 mg/dL. On examination, the patient was unresponsive to verbal commands and decerebrated on deep painful stimuli. Deep tendon reflexes were brisk bilaterally and he had well sustained bilateral ankle clonus with bilateral upgoing plantars. Seizures were hard to control, requiring intravenous phenytoin and phenobarbital loading and finally intravenous midazolam. Cerebral MR done 10 days after presentation showed gyriform increased signal in both the temporal and parietal lobes, suggestive of cortical laminar necrosis [Figure - 1][Figure - 2]. Discussion The gray matter of the cortex has six layers. The third layer is the most vulnerable to anoxia and hypoglycemia. Cortical laminar necrosis is a specific type of cortical infarction, usually seen in the setting of anoxic encephalopathy. Other etiologies like hypoglycemia, status epilepticus and immunosuppressive chemotherapy have been implicated.[1],[2] The appearance of the MR images in the setting of diffuse cortical laminar necrosis can be deceptive. Properly windowed diffusion weighted imaging can be very helpful in detecting cortical laminar necrosis, especially in the setting of anoxic-hypoxic encephalopathy in the early subacute phase.[3] Cortical laminar necrosis in the setting of anoxic encephalopathy has a universally poor prognosis, with most patients either progressing to brain death or remaining in a persistent vegetative state.[2] Our patient too had a poor outcome and remains in a persistent vegetative state.References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06115f2.jpg] [ni06115f1.jpg] |
| |||||||||

{kind=link}
{kind=link}