 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
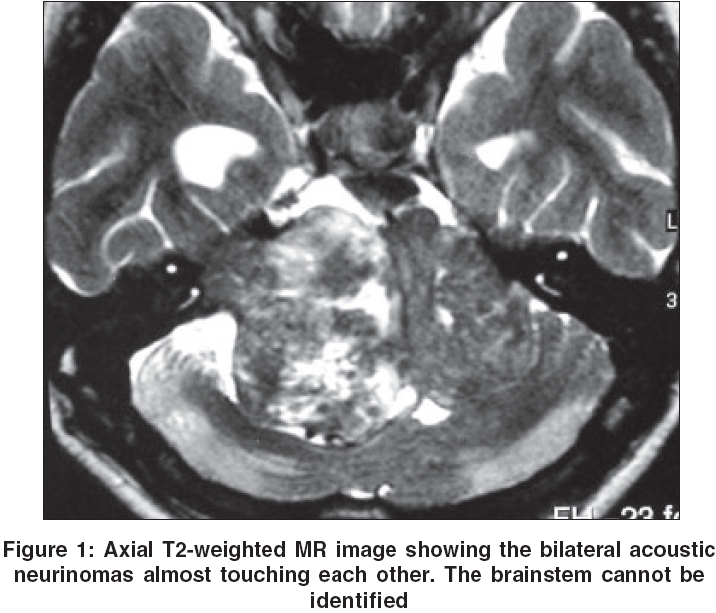
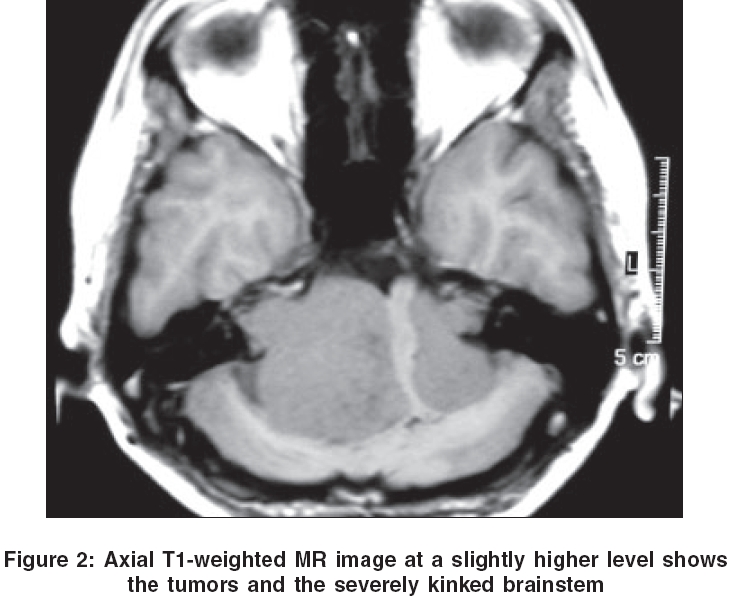
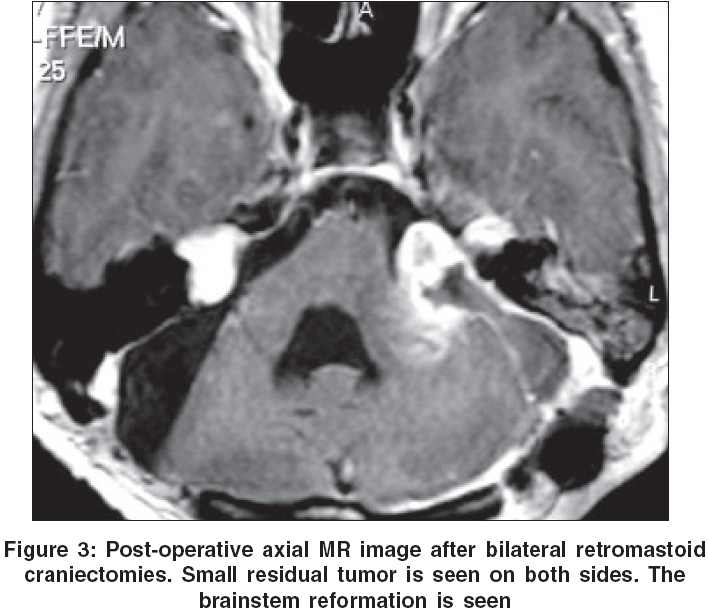
Neurology India, Vol. 54, No. 3, July-September, 2006, pp. 329-330 Neuroimage Bilateral acoustic neurinomas Goel A, Muzumdar D Department of Neurosurgery, Seth Gordhandas Sunderdas Medical College and King Edward VII Memorial Hospital, Mumbai Date of Acceptance: 05-Feb-2006 Code Number: ni06117 A 20-year-old girl with family history of neurofibromatosis presented with complaints of decreased hearing in both ears, change in voice, headaches and progressive ataxia for the past 1 year. On admission, she was alert, active but dysarthric. There was bilateral horizontal gaze evoked nystagmus. Fundus examination revealed bilateral papilledema. The right corneal reflex was depressed and the sensations over the right side of face were marginally decreased. There was right facial paresis, bilateral sensorineural deafness and severe truncal ataxia. There were marked bilateral cerebellar signs. MR imaging showed large bilateral acoustic neurinomas severely compressing the brainstem [Figure - 1][Figure - 2]. It was difficult even to identify the brainstem in certain sequential images. A radical resection of both acoustic neurinomas was performed through bilateral retromastoid craniectomies in two stages at an interval of 3 months. On both sides, a thin sheath of tumor was left behind adjacent to the facial nerves in an attempt to save their function. The patient developed right facial palsy following the first surgery and needed tarsorrhaphy. However, her ataxia improved remarkably. Post-operative MR imaging showed considerable reformation of the brainstem [Figure - 3]. Discussion Bilateral acoustic neurinomas are commonly associated with neurofibromatosis-type 2. The treatment protocol in such cases is controversial and a number of management strategies have been presented in the literature.[1],[2],[3] Our case presented with bilateral deafness, a feature which made surgical decision making relatively easier. The goal of surgery was to radically excise the tumor and to save the facial nerve. However, the function of the seventh nerve could not be preserved, despite the anatomical preservation of the nerve during surgery. The large size of the tumor and its high vascularity probably lead to its damage during dissection. The tumors on both sides were large and almost touched each other and resulted in remarkable distortion of the brainstem. Despite the fact that the brainstem was severely kinked prior to the surgery, it still was in its functional state and majority of the brainstem reflexes were intact. The case demonstrates the functional resilience of the brainstem. The elasticity and anatomical reformation after surgical resection of the tumors are also demonstrated.References
Copyright 2006 - Neurology India The following images related to this document are available:Photo images[ni06117f1.jpg] [ni06117f2.jpg] [ni06117f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}