 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
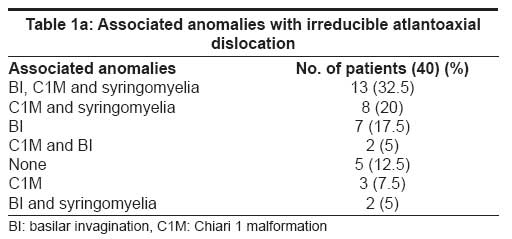
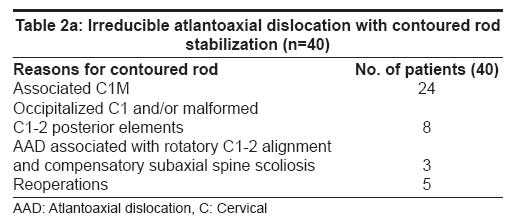
Neurology India, Vol. 55, No. 4, October-December, 2007, pp. 363-368 Original Article Occipitocervical contoured rod stabilization: Does it still have a role amidst the modern stabilization techniques? Samir K. Kalra, Vijendra K. Jain, Awadesh K. Jaiswal, Sanjay Behari Department of Neurosurgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow - 226014, India Date of Acceptance: 11-Jun-2007 Code Number: ni07108 Abstract Background: The occipitocervical contoured rod (CR) stabilization for use in craniovertebral junction (CVJ) pathologies is an effective and economical technique of posterior fusion (PF).Aims: The various indications for CR in CVJ pathologies are discussed. Settings and Design: Retrospective analysis. Materials and Methods: Fifty-four patients (mean age: 31.02 ± 13.44 years; male: female ratio=5.75:1) who underwent CR stabilization are included. The majority had congenital atlantoaxial dislocation (AAD; n=50); two had CVJ tuberculosis; one each had rheumatoid arthritis and C2-3 listhesis, respectively. The indications for CR fusion in congenital AAD were associated Chiari 1 malformation (C1M) (n=29); occipitalized C1 arch and/or malformed or deficient C1 or C2 posterior elements (n=9); hypermobile AAD (n=2); and, rotatory AAD (n=3). Contoured rod as a revision procedure was also performed in seven patients. Most patients were in poor grade (18 in Grade III [partial dependence for daily needs] and 15 in Grade IV [total dependence]); 15 patients were in Grade II [independent except for minor deficits] and six in Grade I [no weakness except hyperreflexia or neck pain]. Results: Twenty-four patients improved, 18 stabilized and six deteriorated at a mean follow-up (FU) of 17.78 ± 19.75 (2-84) months. Six patients were lost to FU. In 37 patients with a FU of at least three months, stability and bony union could be assessed. Thirty-one of them achieved a bony fusion/ stable construct. Conclusions: Contoured rod is especially useful for PF in cases of congenital AAD with coexisting CIM, cervical scoliosis, sub-axial instability and/or asymmetrical facet joints. In acquired pathologies with three-column instability, inclusion of joints one level above the affected one by using CR, especially enhances stability. Keywords: Atlantoaxial dislocation, contoured rod, craniovertebral junction, posterior fusion The craniovertebral junction (CVJ) represents a unique and complex interface responsible for more than half of the rotation and flexion-extension of the cervical spine. The osseous articulations and their supporting ligaments must resist forces in all axes of motion. [1],[2],[3],[4],[5] Various pathological conditions can destabilize this junction. The surgical goal, therefore, is relief of neural compression and stabilization. [6],[7],[8],[9] Occipitocervical fusion was first described by Forrester in 1927. [9] All internal fusion techniques focus on providing rigid constructs to facilitate bony fusion and reduce the need for and the duration of external immobilization. [2],[3],[5],[7],[9],[10],[11] The various techniques of posterior stabilization of CVJ are classified into those that use 1) Methylmethacrylate; 2) Occipitocervical plates and screws; 3) Contoured rod (CR) with wires; 4) Metallic clamps; and, 5) Trans-articular screws. Autologous bone graft promotes a good bony union. The long-term stabilization depends on bony integration. [10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20] The Ransford′s occipitocervical CR fusion method first reported in 1986 has stood the test of time as an effective and economical method of posterior stabilization. [19] The technique involves fixing a prefabricated loupe to the occiput and the upper cervical laminae using sublaminar wires. [6],[8],[9] The first description of the technique in India was by Das et al . [12] The basic method has remained constant albeit with minor modifications including threaded pins, interspinous wiring, shape variations and the use of magnetically inert materials. [9],[11],[14],[20],[21] Despite the emergence of several new occipitocervical fusion techniques,[8],[9],[10],[15],[17],[22],[23] CR fusion is still one of most economical and versatile methods that is especially useful in certain specific situations. This study focuses on the indications, outcome, advantages and drawbacks in using CR fusion. Materials and Methods Patient spectrum Fifty-four consecutive patients (mean age: 31.02 ± 13.44 years; range 3-65 years; male: female ratio=5.75:1) who underwent CR fusion in past 10 years (January 1997 to 2006) were included and analyzed retrospectively. The complete patient information was recorded prospectively on prescribed proformas as a part of ongoing protocol on CVJ pathologies. The majority of them had congenital atlantoaxial dislocation (AAD; n=50). Their associated anomalies are presented in [Table 1a and b]. The indications for using CR were coexisting Chiari 1 malformation (C1M) (n=29); occipitalized C1 arch and/or malformed or deficient C1 or C2 posterior elements (n=9); hypermobile AAD (n=2); and, rotatory AAD with compensatory subaxial scoliosis (n=3). Also included were those patients who underwent CR during revision surgery (n=7). Two patients having irreducible AAD with basilar invagination (BI), C1M and syringomyelia underwent posterior decompression at another center [Figure 1]a and b. Following their neurological deterioration at follow-up, a transoral decompression (TOD) and CR stabilization was performed. Three patients with irreducible AAD and BI underwent transoral surgery with occipitocervical fusion using Jain′s technique. [1],[3] They did not improve due to residual posterior bony compression (n=2); or, both anterior and posterior bony compression (n=1). The patients who had previously undergone only posterior decompression underwent a repeat posterior stabilization using CR. The one patient who had previously undergone both anterior and posterior decompression underwent a revision single-stage TOD and CR. Two patients having reducible AAD also underwent a revision CR fusion. One of them had associated C1M with syringomyelia for which posterior decompression had already been performed elsewhere. He underwent CR stabilization due to persisting reducible C1-2 dislocation. The other patient had an initial posterior C1-2 sublaminar fusion and did not improve. His intrathecal contrast enhanced computed tomographic scan (ITCT) revealed residual cord compression from the posterior aspect. The posterior margin of the foramen magnum and the artificial arch were excised and a CR placed [Table 2a and b] The acquired (n=4) conditions included tuberculous AAD [Figure 2] a, b, c and d (n=2); rheumatoid AAD (n=1); and traumatic C2-C3 listhesis [Table 2c]. The patients were clinically graded as: [1],[24] Grade I: independent without deficits except with hyperreflexia or neck pain (n=6); Grade II: minor deficits but independent for daily needs (n=15); Grade III: partially dependent on others for daily needs (n=18); and, Grade IV: totally dependent (n=15). Improvement or deterioration was considered on the basis of changes in grades. Radiology The radiological investigations included plain dynamic CVJ radiographs (neutral, flexion and extension) and cranio-spinal MRI. The postoperative ITCT imaging was used to determine adequacy of reduction, amount of decompression and stabilization. A postoperative MRI was not possible due to the use of stainless steel constructs. Forty patients had irreducible AAD (patients who did not achieve reduction of AAD on extension or following traction) and 10 had reducible AAD. Basilar invagination was evaluated using McRae′s line, Wackenheim′s clival canal line, McGregor′s line and Chamberlain′s line. [1],[3],[5],[16],[25],[26] The extent of soft tissue involvement was noted in patients with tuberculous (n=2) and rheumatoid (n=1) affliction. [16],[25],[27],[28],[29],[30] Primary surgical management A preoperative Crutchfied′s cervical traction was placed in our patients. All except three patients with irreducible AAD underwent TOD prior to the posterior procedure. The latter three patients also required a subsequent TOD following neurological deterioration at follow-up. [3],[18],[31],[32] In the two patients with tuberculous AAD and the one with rheumatoid AAD, TOD removed the tuberculous granulation or rheumatoid pannus, respectively. [16],[27],[29],[30],[34] The occipitocervical fusion included Oc-C3 vertebral levels in 19 (35.2%), Oc-C4 levels in 25 (46.3%) and Oc-C5 levels in 10 (18.5%) patients [Table 3]. Operative technique The anterior decompression was performed in the supine position through the standard transpalatal, transpharyngeal route [1],[3],[18],[26],[32],[33] followed by CR under the same anesthesia. A non-threaded, stainless steel Steinmann pin (4-5 mm diameter) was shaped and fixed to the occipital squama and the upper cervical laminae using braided Aesculap No. 5 stainless steel wires (Ethicon, Johnson and Johnson). Onlay autologous rib grafts were also placed [Figure 3]a, b and c. The construct cost was approximately 500 rupees (12 US dollars). Postoperative management Early ambulation was encouraged and hard cervical collar was worn for minimum of three months. The stabilization was assessed by visualizing a firm contact of the ends of the graft with bony occipitocervical surfaces (with or without new bone formation) without relative movement in flexion-extension radiological studies, at three months or more [Figure 4]. The serial clinico-radiological evaluations were performed at discharge and at follow-up visits (three months, six months and then at yearly intervals) The patients having tuberculosis were continued on anti-tubercular treatment (18 months); and, the one with rheumatoid arthritis was continued on anti-rheumatoid therapy. [27],[35] Results There were 15 patients in Grade II, 18 in Grade III and 15 in Grade IV. Only six were preoperatively in Grade I. Three of the latter group had an irreducible AAD, C1M and syringomyelia with a history of transient quadriparesis following minor trauma that improved subsequently with residual spasticity and/or hyperreflexia. The other three patients had reducible AAD (one each having hypermobile AAD; associated C1M and syringomyelia; and deficient posterior C1-2 elements). Following surgery, 24 patients improved, 18 stabilized, four deteriorated and two died at the mean follow-up of 17.78 ± 19.75 (range: 2-84) months [Table 4]. Six (11.1%) patients were lost to follow-up. Among the four patients with deterioration, one had hypermobile AAD, was in preoperative Grade I and developed minor deficits. The other three patients (one with reducible AAD, C1M and syringomyelia; two with irreducible AAD) were in preoperative Grade II. All three had initially undergone sublaminar fusion, had persisting posterior compression and improved following decompression and CR stabilization. The two mortalities occurred in Grade IV patients with irreducible AAD, C1M and syringomyelia with severe respiratory compromise who succumbed to bronchopneumonia. There were 37 patients out of 46 patients (excluding six lost to follow-up and two deaths) with a follow-up long enough to assess for bony fusion (three months post-surgery). Thirty-one (83.8%) of these patients achieved a stable bony fusion. All the seven patients who underwent CR as a repeat procedure showed improvement. Nine patients in the series required a tracheostomy that was maintained for two to 22 months. The postoperative complications included wound gape following TOD (n=4). They were managed conservatively and improved. There was vertebral artery injury with pseudoaneurysm formation in one patient with rheumatoid arthritis during the TOD. The complications following the posterior procedure were cerebrospinal fluid (CSF) leak in four and construct infection in two patients. Discussion Technical considerations The inclusion of the occiput in the posterior fusion enhances stability in cases where extensive osteoligamentous destruction and/or instability of the occiput and upper cervical vertebrae coexist. [11],[19],[24],[27] In our patients with irreducible AAD, there was often an occiput- C1 and C2-3 fusion. In patients with tuberculous or rheumatoid affliction, there was a simultaneous lateral joint involvement. A summary of the various occipitocervical fusion techniques is presented in [Table 5]. [21],[32] The CR proved to be an effective and inexpensive method of providing a rigid stabilization. [36],[37],[38],[39] Significant kyphosis or scoliosis could be compensated for without significant sublaminar compression. [4],[14],[19],[24],[38] There is a negligible risk of vertebral artery injury. The modern techniques, however, may have greater stability and CR has mechanical limitations in maintaining spinal alignment and deformity correction. It requires an intact lamina for fixation; does not include the afflicted spinal level; requires longer fusion than decompression levels; and has the potential risk of dural penetration by wires. Most patients had congenital AAD and the lateral joints were frequently asymmetrical with often vertically oriented occipito C1-2 facets. In another series, 78.6 % of pediatric patients with congenital AAD had asymmetrical or vertical joints. [40] In these situations, newer methods involving lateral masses or transarticular screws have higher risk of abnormal placement of the construct. Even with normal joints, the incidence of arterial injury or faulty placement is high (2-5% in various series). [5],[15],[22],[41],[42] Considerations in congenital anomalies The extent of anterior resection may vary from from drilling the clivus in BI to removal of the C2-3 body and this determines the levels of elements included during posterior fusion. [1],[3],[32] We usually performed modified Brooks′ technique for reducible AAD. [1],[3],[33] In some of these patients, however, the amount of neck extension required to achieve an adequate C1-2 reduction may severely compromise the desired area of surgical exposure. In CR stabilization, the neck may be maintained in neutral postion with an in situ stabilization of the vertebral bodies performed. In the two patients with hypermobile AAD with os odontoideum, CR was considered safer than the Brooks′ technique as there was danger of the posterior C1 arch being pulled backwards into the cervical canal in the latter technique. Considerations in acquired pathologies Behari et al. [27] have recommended conservative management in good grade and aggressive surgical therapy for poor grade patients with tuberculous AAD. Gupta et al. , [6] in fact, have recently questioned the need of surgery. Nannapaneni et al. [29] and Crockard [31],[43] have emphasized increased incidence of short segment fusion failure in rheumatoid affliction. With extensive osteo-ligamentous destruction, CR stabilization helps in achieving a long segment fusion. During TOD in our case, of rheumatoid AAD, the medially displaced vertebral artery was inadvertently injured. The resultant traumatic pseudoaneurysm had to be coiled. Fortunately, there were sufficient collaterals and the patient had no deficits. Considerations during revision surgery Patients with C1M should be investigated for an associated AAD. [5] Three such patients underwent only posterior decompression at another center. Following neurological deterioration those with irreducible AAD (n=2) underwent TOD and CR and the one with reducible AAD underwent CR stabilization. Three patients with residual compression following sublaminar wiring required repeat decompression and CR placement. It is reported that long segment constructs cause a 10- to 20- degree loss of lateral bending, flexion-extension and axial rotation. [6],[9],[11],[13],[14],[19],[36],[37] In our patients with congenital AAD, this was not disabling as movements were already restricted due to asymmetric or hypoplastic facet joints. In patients with acquired disorders, severe pain, muscle spasm and lateral joint involvement had already severely restricted neck movements. [38],[39] To conclude, CR stabilization forms an economical, simple and effective method of occipitocervical stabilization. In cases of asymmetrically disposed or diseased facet joints and lateral masses this method may in fact be the best way of securing stability.[47] References
Copyright 2007 - Neurology India The following images related to this document are available:Photo images[ni07108t2c.jpg] [ni07108f1.jpg] [ni07108f2.jpg] [ni07108f4.jpg] [ni07108f3.jpg] [ni07108t1b.jpg] [ni07108t2a.jpg] [ni07108t1a.jpg] [ni07108t2b.jpg] [ni07108t3.jpg] [ni07108t5.jpg] [ni07108t4.jpg] |
| |||||||||

{kind=link}
![b]](/showimage?ni/photo/ni07108t1b.jpg){kind=link}
![[Figure 1]](/showimage?ni/photo/ni07108f1.jpg){kind=link}
{kind=link}
![b]](/showimage?ni/photo/ni07108t2b.jpg){kind=link}
![[Figure 2]](/showimage?ni/photo/ni07108f2.jpg){kind=link}
![[Table 2c]](/showimage?ni/photo/ni07108t2c.jpg){kind=link}
![[Table 3]](/showimage?ni/photo/ni07108t3.jpg){kind=link}
![[Figure 3]](/showimage?ni/photo/ni07108f3.jpg){kind=link}
![[Figure 4]](/showimage?ni/photo/ni07108f4.jpg){kind=link}
![[Table 4]](/showimage?ni/photo/ni07108t4.jpg){kind=link}
![[Table 5]](/showimage?ni/photo/ni07108t5.jpg){kind=link}