 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
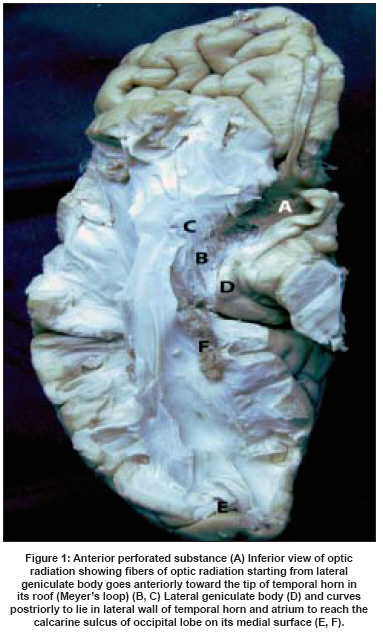
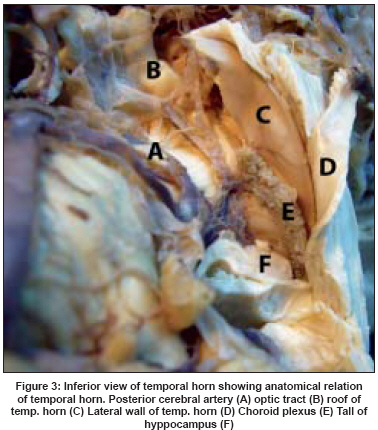
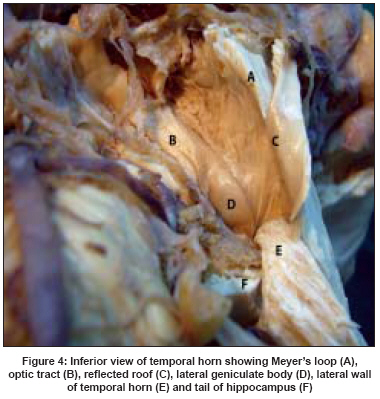
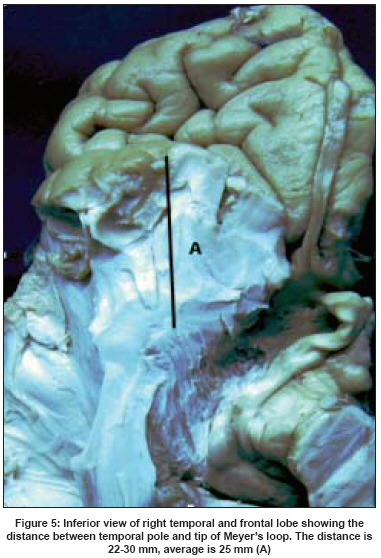
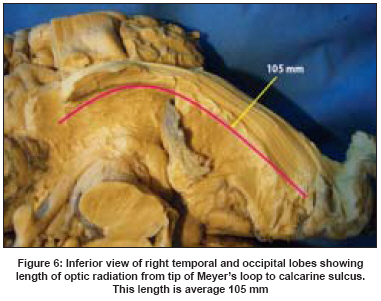
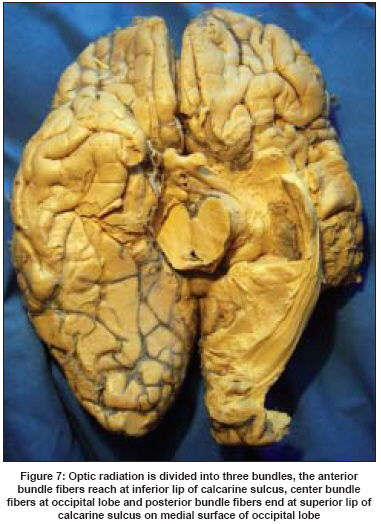
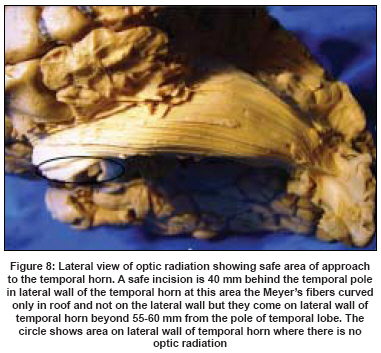
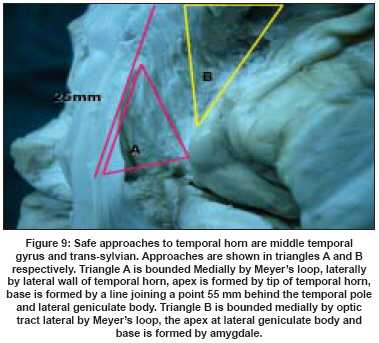
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 133-137 Original Article Fiber dissection of the visual pathways: Analysis of the relationship of optic radiations to lateral ventricle: A cadaveric study Pujari VikrantB, Jimbo Hiryuki, Dange Nitin, Shah Abhidha, Singh Sukhdeep, Goel Atul Department of Neurosurgery, King Edward Memorial Hospital and Seth G.S. Medical College, Parel, Mumbai Code Number: ni08039 Abstract Objective: Using a fiber-dissection technique, our aim is to study the fiber bundles of the optic radiation. We focused on the course, the length, anatomical relations with lateral ventricle and the relevance of these finding during surgery in the region.Materials and Methods: Five previously frozen and formalin-fixed cadaveric human brains were used. The dissection was done using the operating microscope. Fiber dissection techniques described by Klingler were adopted. The primary dissection tools were handmade, thin, and wooden and curved metallic spatulas with tips of various sizes. Lateral and inferior temporal approaches were made and the optic fiber tracts were dissected. Results: Resections that extend through the roof of the temporal horn more than 30 mm behind the temporal pole cross the Meyer's loop. In the middle temporal gyrus approach, resection that is taken through the lateral wall of the temporal horn more than 55-60 mm behind the temporal pole may cross the optic radiation during their course here on the lateral wall. Conclusion: The presented fiber dissection study clarifies the relationship of optic radiation. Such fiber dissection studies are only few in the literature. Keywords: Fiber dissection, Meyer′s loop, microsurgical anatomy, optic radiation, temporal lobe Introduction In temporal lobe region surgery, for tumors and epilepsy, the exact anatomical relationship of the optic tract fibers to temporal horn are inadequately visualized on conventional cadaveric brain dissection. Fiber dissection of the brain delineates the anatomical details of the tracts clearly and assists in providing a 3-dimensional perspective. Only a few studies are available in the literature concentrating on fiber dissection of the brain in general and on optic tracts in particular. [1],[2],[3],[4],[5] The surgical approach to temporal horn and mediobasal structures can be categorized into three main groups: lateral, subtemporal and transsylvian. [6] These approaches have their own merits and demerits based on location of language and visual processing areas in the lateral temporal lobe and underlying the fibers including the optic radiations. In this presentation, we attempt to evaluate the anatomical relationships of optic radiations and advantage of approach to temporal horn through safe area of lateral wall of temporal horn. Materials and Methods Five normal human cerebral hemispheres were fixed in formalin for forty days and then frozen at the temperature of 10-15 degrees Celsius for fourteen days. We dissected these specimens under the operating microscope (with 6X to 40X magnification) using the fiber-dissection techniques initially described by Klingler. [7] The primary dissection tools were handmade, thin, and wooden and curved metallic spatulas with tips of various sizes. Lateral and inferior temporal approaches were made to expose the region. The inferior part of the temporal lobe and floor of temporal horn including short and long association fibers, head, part of body of hippocampus, fimbria, amygdala were removed. Fibers of optic radiation in the roof and the lateral wall of temporal horn were exposed by removing the ependymal layer. With further dissection optic radiation fibers were followed into the lateral geniculate body and to the occipital cortex. The distance between tip of Meyer′s loop and temporal pole, length and breadth of the optic radiation from tip of Meyer′s loop to calcarine fissure was measured.Results The optic radiations extended from the lateral geniculate body to the occipital cortex [Figure - 1]. Anatomical relation of Meyer′s loop with adjacent structures is shown in [Figure - 2],[Figure - 3],[Figure - 4]. Distance from temporal pole to tip of Meyer′s loop was 22 to 30 mm (average of 25 mm, [Figure - 5]). The average length of the optic radiation from the tip of Meyer′s loop to the calcarine fissure was 105 mm. The breadth of the optic radiation was 17 mm and it enlarged towards to occipital pole [Figure - 6]. The distance from tip of Meyer′s loop to the point where optic radiation curves on the lateral wall of temporal horn were identified to be 25 to 30 mm and the distance from temporal pole to this point was 55 to 60 mm. The distance between tip of Meyers loop and important landmarks in average are shown in [Figure - 1],[Figure - 2],[Figure - 3],[Figure - 4],[Figure - 5],[Figure - 6],[Figure - 7],[Figure - 8],[Figure - 9].Discussion Visual pathways originate from temporal half of ipsilateral retina as nerve fibers of optic tract, which begins at posterolateral corner of optic chiasma, pass posterolaterally between anterior perforated substance and tuber cinereum. These fibers lie superior to medial aspect of temporal lobe on lateral aspect of crus cerebri. On the crus cerebri, the optic tract is close to the choroidal fissure of inferior horn of lateral ventricle and is crossed by the anterior choroids branch of the internal carotid artery on its way to fissure, and by the basal vein passing around the midbrain to great cerebral vein. Each optic tract enters the corresponding lateral geniculate body appearing to divide into two roots. The medial root seems to pass to medial geniculate body, but the only fibers which continue posterior to lateral geniculate body are those of the brachium of the superior colliculus which run in the interval between the two roots to the superior colliculus. Each optic tract contains nerve fibers which originate from temporal half of ipsilateral retina and the nasal half of the contralateral retina. Optic radiation starts at lateral geniculate body, proceeds posteriorly by dividing into three bundles, anterior or Meyer′s loop, [8] central bundle and posterior bundle. These fibers lie in sublenticular and retrolenticular parts of internal capsule and then curve around the temporal horn and atrium. Subsequently, these fibers are separated from ventricle surface by thin layer of tapetal fibers. Anterior bundle fibers reach at inferior lip of calcarine sulcus, center bundle fibers at occipital lobe and posterior fibers end at superior lip of calcarine sulcus on medial surface of occipital lobe [Figure - 7]. The study revealed that the distance from temporal pole to tip of Meyer′s loop is average 25 mm, any resections that extend through the roof of the temporal horn more than 30mm behind the temporal pole cross the Meyer′s loop. The distance from temporal pole to a point where optic radiation curves on lateral wall of temporal horn is 55 to 60 mm, any resection that is taken through the lateral wall of the temporal horn more than 55-60 mm behind the temporal pole may cross the optic radiation as they curve here on lateral wall. Contralateral superior quadrantanopia has been reported to occur in approx.50% of patients after temporal lobectomy. [9],[10],[13],[14],[15] Transtemporal and trans-sylvian approaches are commonly used for amygdala-hippocampectomy. [11],[12] Middle temporal gyrus approach to the temporal horn has a low risk of damaging the Meyer′s loop if incision is made 40 mm behind the temporal pole in lateral wall of the temporal horn at this area the Meyer′s fibers curved only in roof and not on the lateral wall but they come on lateral wall of temporal horn beyond 55-60 mm from the pole of temporal lobe. The circle in [Figure - 8] shows area on lateral wall of temporal horn where there is no optic radiation. Temporal horn can also be entered through the floor of sylvian fissure from a triangle without damaging the optic radiation. This triangle is bounded medially by optic tract, laterally by Meyer′s loop, the apex is at the lateral geniculate body and base is formed by amygdaloid nucleus [Figure - 9]. Radiological techniques such as MRI and reconstructed diffusion tensor fiber tractography of the optic radiation can be used preoperatively to avoid damage to optic radiation during temporal lobe surgery, because in some cases anterior fibers of Meyer′s loop curve more anteriorly so that the distance between the temporal pole and tip of Meyer′s loop is reduced to less than 25 mm. This fiber dissection study is beneficial to increase our knowledge of brain anatomy, which is essential for neurosurgical approaches to avoid a damage of the optic radiations. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08039f8.jpg] [ni08039f4.jpg] [ni08039f6.jpg] [ni08039f1.jpg] [ni08039f9.jpg] [ni08039f5.jpg] [ni08039f2.jpg] [ni08039f3.jpg] [ni08039f7.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}