 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
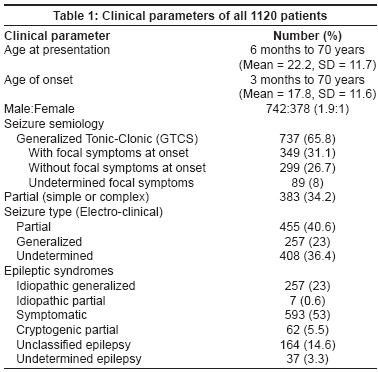
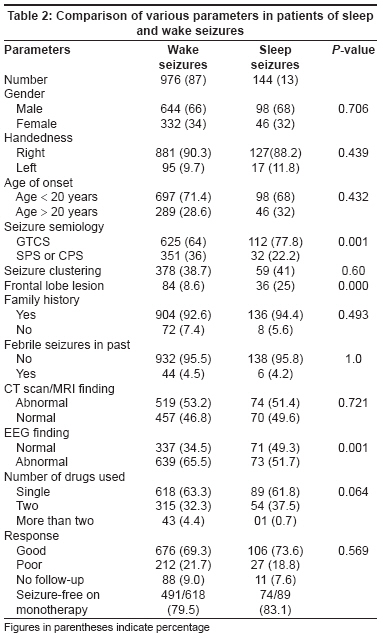
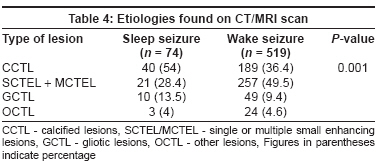
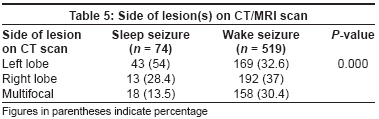
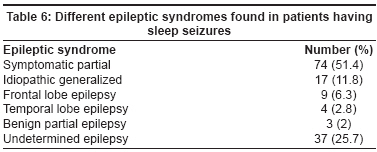
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 151-155 Original Article Sleep seizures versus wake seizures: A comparative hospital study on clinical, electroencephalographic and radiological profile Goel Deepak, Mittal Manish, Bansal KK, Srivastav RK, Singhal A Department of Neurology, Himalayan Institute of Medical Sciences, Dehradun Code Number: ni08042 Abstract Background: Epileptic seizures, predominantly or exclusively during sleep had been the focus of attention for many electroencephalographers. Though few epileptic syndromes are associated with sleep seizures (SS) its frequencies in Indian patients is still unknown.Aim: To find out the patterns of epilepsies in patients having SS and compare them with patients having wake seizures (WS). Setting and Design : Open label hospital based study. Materials and Methods: One hundred and forty-four (13%) patients having predominantly SS were compared with 976 (87%) patients of WS by various clinical, electrophysiological and radiological factors. Statistical Analysis: Chi square test and student T test, using software SPSS (version 10, 1999) was applied to compare various parameters. Relative risk was calculated by 2 x 2 contingency table. Results: The seizure semiology was better defined in patients with WS and GTCS was more common in SS ( P = 0.001). Wake-electroencephalogram (EEG) was abnormal in significantly ( P = 0.001) higher number of patients with WS. Symptomatic etiologies were found in more than half patients. Left lobe involvement was more common in patients having SS ( P = 0.000). After symptomatic, idiopathic generalized and frontal lobe epilepsy were most frequent with SS. Undetermined epilepsy was found in 37 (25.7%) patients with SS. Conclusion: Epilepsies associated with SS were less frequent and had symptomatic cause in most cases. Left hemispherical and frontal lobe lesion were more commonly associated with SS. Frontal lobe and idiopathic generalized epilepsy was most frequent in patients of SS. Sleep EEG should always be done in patients with sleep seizures. Keywords: Epilepsy in India, frontal lobe epilepsy, sleep epilepsy The International League Against Epilepsy (ILAE) defined sleep seizures (SS) as "seizures occurring exclusively or predominantly (more than 90%) during sleep". [1] Proportion of patients with SS ranges from 7.5 to 45% (average 12%) in different studies. [2],[3] Sleep has an important role in triggering seizures and electroencephalographic abnormalities in both idiopathic (i.e. idiopathic generalized epilepsies, rolandic epilepsy, nocturnal frontal lobe epilepsy [NFLE]) and symptomatic (polimicrogyria and continuous spike-waves in sleep) epileptic syndromes. [4],[5] Therefore clinical history about seizures should always include information about the time of seizure occurrence. This is particularly important in children where such clinical information can be the determinant for syndromic diagnosis and prognosis of epilepsy. However, only trained epileptologists give emphasis on the timing of seizures in the clinical history of an epileptic patient. Most of the literature available on sleep epilepsy is from the western world where etiologies are different from tropical countries. No Indian data is available about the proportion and type of epileptic syndromes associated with sleep seizures. Secondly we don′t know how the patients of sleep seizures behave differently from patients with wake seizures in clinical parameters. Therefore this study was conducted to fill this paucity of data about sleep epilepsy from tropics. Materials and Methods This study was conducted in the neurology department of a tertiary care center located in the northern hilly part of India. All patients presenting with recurrent seizures since 2002 up to 2006 were included. The SS were defined as per the ILAE definition; [1] recurrent epileptic seizures occurring exclusively or predominantly [>90%] during sleep, with a stable nocturnal seizure pattern from the time of seizure onset until time of last follow-up. A total of 1300 patients attending the outpatient department of our unit were evaluated. One hundred and eighty patients with febrile convulsions, single seizure, neonatal or infantile seizures and severe mental/physical disability were excluded. A total of 144 patients (13%) presenting with SS were compared with 976 (87%) patients with most seizures in wakeful state (WS). Comparison was based on the following parameters: the clinical and demographic profile like age, age at onset of seizures, handedness, seizure semiology (GTCS, focal or unclassified/undetermined), episodes of seizures in cluster (yes/no), history of febrile convulsions, family history of seizure disorders, abnormalities on electroencephalogram (EEG) and imaging [computerized tomography (CT) scan or magnetic resonance imaging (MRI)] and epileptic syndromes. As per protocol CT scan was done in all patients at the time of first evaluation along with EEG. The MRI was only advised when there was definite semiological evidence of symptomatic cause and CT scan had normal findings. The EEG abnormality was defined into four categories: (1) generalized epileptiform, (2) focal epileptiform, (3) non-epileptiform abnormalities and (4) normal EEG after 30 min wake recording. Side and nature of lesion on post-contrast CT scan or MRI was recorded. Findings were classified as CCTL - Calcified lesions, SCTEL/MCTEL - single or multiple small enhancing lesions, GCTL - gliotic lesions, OCTL - other lesions (developmental, cortical dysplasias, mesial temporal sclerosis). Side of lesion on imaging was described as left lobe or right lobe involvement in case of single discrete lesion and multifocal when more than one lobe was involved. Number of cases having isolated frontal lobe lesion were recorded in both groups. Different seizure types and epilepsy syndromes were classified according to standard international classifications by ILAE. After evaluation patients were treated with antiepileptic monotherapy according to seizure type. First antiepileptic given in patients of partial seizures was either phenytoin sodium or carbamazepine, while sodium valproate or phenobarbitone was given to the patients of generalized or undetermined seizures type. Response to antiepileptic was recorded as good (complete or more than 50% reduction in seizures) or poor (no or less than 50% reduction in seizures during follow-up) with minimum follow-up period of 12 months. Patients were followed up monthly for the first six months and then at every three months. Follow-up evaluation was conducted either by personal visit or telephonically. Statistical analysis between different clinical, radiological and electrophysiological parameters was done by Chi square test and Student′s t test, using software SPSS (version 10, 1999). Relative risk was calculated by 2 x 2 contingency table. Odd Ratio (OR) more than 1 with lower limit of Confidence Interval (CI) more than 1 was taken as significant. Results Age of presentation, age of onset, seizures types and epilepsy types of all 1120 patients are presented in [Table - 1]. Comparison of clinical, radiological and electrophysiological parameters in the two groups is shown in [Table - 2]. No significant difference was found between the two groups in age of onset, sex ratio, handedness, seizure clustering, family history, old febrile convulsions, radiological findings, number of antiepileptics used and response to treatment. Among the antiepileptics used carbamazepine was the most commonly prescribed antiepileptic in both the groups, but phenobarbitone was prescribed for a significantly higher proportion of patients with SS. The semiology of WS was better defined in comparison to SS. Overall, 732 (65.4%) patients had evidence of focal onset seizures on semiological basis. Primary or secondary generalized tonic-clonic seizure (GTCS) was the most common type in both groups with 625 (64%) patients in the WS and 112 (77.8%) in the SS group ( P = 0.001). History of focal symptoms at onset of GTCS was identified in 326 (52.1%) patients with WS while only 23 (20.5%) patients with SS could give such history. Simple partial or complex partial semiology was present in 351 (36%) and 32 (22.2%) patients with WS and SS respectively. Overall EEG findings were abnormal in 73 (51.7%) patients of SS and in 639 (65.5%) patients of WS ( P = 0.001). In patients with normal CT scan, the proportion of normal/nonspecific EEG findings was further high in patients with SS 37/70 (52.9%) than in patients with WS [164/457 (33.3%)] [Table - 3]. The electro-clinical classification of seizures by ILAE was applicable to only 712 (63.6%) patients as in 408 (36.4%) patients finding of the first wake-EEG was noncontributory. The CT scan was done in all patients but MRI could be done only in 120 (10.7%) patients. The CT scan/MRI was abnormal in 74 (51.4%) and 519 (53.2%) patients with SS and WS respectively ( P = 0.72). Different types of lesions on CT scans/MRI are presented in [Table - 4]. Active or healed brain infection (neurocysticercosis) accounted for radiological abnormalities in most of the cases. The left lobe involvement was significantly higher with SS in 43 (54%) patients in comparison to 169 (32.6%) patients with WS ( P = 0.0003) [Table - 5]. Isolated frontal lobe lesion was present in 84 (8.6%) and 36 (25%) patients with WS and SS respectively ( P ≤ 0.0001). Relative risk of sleep seizure in patients with left lobe lesion (OR = 2.03 and CI = 1.37-3.01) and frontal lobe lesion (OR = 2.66 and CI = 1.73 to 4.07) was significantly high. Different epilepsies in patients with sleep seizures are shown in [Table - 6]. Symptomatic epilepsies were almost equal in 519 (53.2%) patients with WS and in 74 (51.4%) patients with SS ( P = 0.7). Idiopathic generalized epilepsies were higher in proportion among patients with wake seizures [238 (24.4%) when compared with SS [17 (11.8%)] ( P = 0.001). Cryptogenic partial epilepsy was diagnosed in 54 (5.5%) patients and one had benign occipital epilepsy in the WS group. Thirteen (9.1%) patients with sleep seizures had cryptogenic 9 (6.3%) had frontal lobe epilepsy and 4 (2.8%) had temporal lobe epilepsy) and 3 (2%) had idiopathic partial epilepsy. Undetermined epileptic syndrome was found in 37 (25.7%) patients with SS and 164 (16.8%) patients with WS had unclassifiable epilepsy ( P = 0.001). Discussion The proportion of patients presenting with sleep seizures is variable but usually around 12.5% as found in the current study. [3] Patients presenting with sleep or wake seizures had almost similar demographic profile. Mean age of patients at onset in our cohort was similar to another multicentric trial from India. [6] On semiological description GTCS was the most frequent type and overall two-thirds of the patients had focal symptoms at onset of seizures. However, semiology-based classification is only a crude method to assess the seizure types and interpretation may be changed after EEG. After awake-EEG in our study partial epileptiform abnormalities were found only in 40.6% patients. Other study by Shah et al. , in pediatric cases and by Joshi et al. , in all age groups had reported partial seizures in 55.3% and 80% of patients respectively in their series. [7],[8] Unclassifiable seizures after EEG testing were much higher in our series in comparison with an older study. [7] The most likely justification was that we could do only awake-EEG due to pressure of doing large number of EEGs in a busy clinic. There are definite evidences that diagnostic yield of EEG in epilepsy specially associated with sleep seizures can be increased by overnight sleep or sleep-deprived record. [9],[10] Due to cost factor limited numbers of MRI scans were performed in our study, however, we could diagnose symptomatic epilepsy in more than half of our patients mainly based on CT scan findings similar to other hospital studies from India. [11],[12],[13] Why only a small proportion of patients threw seizures during sleep is not clear. Our data revealed that patients with left-sided lesion had higher risks of seizures during sleep. Although we have not done detailed testing to determine side of cerebral dominance most of our patients were right-handed and we can presume that patients with dominant lobe pathology might have more chances of sleep seizures. This hypothetical relation of sleep seizure with left-sided lesions had also been supported by a few electrophysiological studies. It is well known that sleep seizures mostly occur during non-rapid eye movement (NREM)-sleep and rarely during rapid eye movement (REM) sleep. [14] One other study had found that these two sleep states are regional processes with NREM being left while REM being right hemispherical predominant. [15] Therefore, left lobe abnormality, NREM sleep and seizures in sleep should have some interrelation. Secondly, sleep deprivation and a few cognitive activities like non-verbal planning, thinking or verbal fluency, during wakefulness have shown to induce slow-waves activity mostly in the left frontal area during NREM sleep and this slow-wave activity is closely related with seizure onset during sleep. [16],[17],[18] However, the relationship between sleep seizures and dominant lobe lesion needs further confirmation with a well-designed polygraphic study. Lesion in the frontal lobe was also more commonly found to be associated with seizures during sleep in our study. There are enough evidences that frontal lobe abnormality is more likely to produce seizure during sleep. [19] We have found that one-fourth patients with sleep seizures had frontal lobe lesion on imaging and a few others had EEG abnormality suggestive of frontal lobe focus. Moreover, we feel that a good number of the FLE cases must have been missed in our analysis as frontal lobe epileptic discharges are difficult to detect on routine wake-EEG testing. [19],[20] Idiopathic Generalized Epilepsy (IGE) in our study commonly presented with both sleep and wake seizures although wake seizures were more likely. Seizures in IGE have strong relation with sleep-wake cycle and tend to occur early in the morning after awakening. One subgroup in epilepsy of grand mal on morning awakening (EGMA) can present with predominant sleep seizures (EGMS). [2] Idiopathic generalized epilepsy, after symptomatic partial, was the second commonest epilepsy in about one-fourth patients reported from India. [7] Thus even though a small fraction (6.6%) of IGE patients had presented with sleep seizures they resulted in a large fraction (11%) of all sleep-related epilepsy cases. Sleep seizures are also common in some symptomatic generalized epilepsy like Lennox-Gastaut Syndrome (LGS) but we had already excluded the cases of epileptic encephalopathy so none was diagnosed in our series. Benign localization-related epilepsies (BLRE) are specially associated with sleep seizures. [21] Only 2% of our patients had BLRE probably due to lesser number of pediatric patients and lack of sleep EEG recording in our study. Around a quarter of patients with sleep seizures had undetermined epilepsy. An antiepileptic drug selection in patients of sleep seizures is easy with specific syndromic diagnosis, as nocturnal FLE is especially responsive to carbamazepine while IGE to valproate, but it is difficult with unclassified disease. Our patients of nocturnal GTCS with undetermined generalized or partial onset were treated with single bedtime doses of broad-spectrum antiepileptics. Although we had not studied the impact of seizures′ timing on patient′s life, overall drug response in terms of seizure remission was similar in patients of both groups. Therefore, even after some methodological limitation our study has grossly represented the profiles of epilepsy with sleep or wake seizures in our setup. To summarize, the proportion of epilepsies with sleep seizures is low. Challenges in diagnosis are more difficult in patients with sleep seizures. The question about the timing of seizures helps in the identification of a few important epilepsies, which otherwise can be missed like frontal lobe and benign epilepsies. It is likely that dominant side and frontal lobe involvement in symptomatic epilepsies is associated with higher number seizures during sleep. The seizures type and epilepsy patterns were difficult to identify in many patients of SS. Techniques like sleep EEG, sleep deprived EEG and video-EEG telemetry are supposed to improve outcome in the diagnosis of patients with SS. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08042t3.jpg] [ni08042t4.jpg] [ni08042t2.jpg] [ni08042t1.jpg] [ni08042t5.jpg] [ni08042t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}