 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
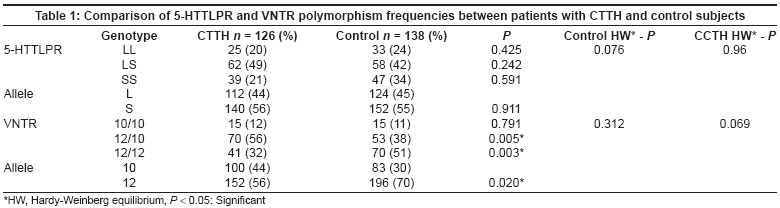
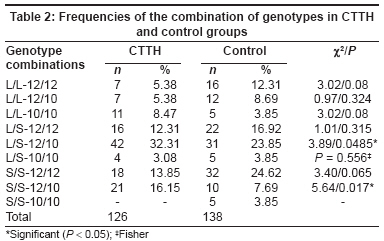
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 156-160 Original Article Serotonin transporter gene polymorphisms in patients with chronic tension-type headache: A preliminary study Akcali Aylin, Tataroglu Cengiz, Erdal Emin, Aydin Neriman, Pehlivan Sacide Department of Medical Biology and Genetics, Gaziantep University, School of Medicine Code Number: ni08043 Abstract Background and Objectives: This study is designed to understand the pathophysiology of one of the most serious health problems, chronic tension-type headache (CTTH). Two polymorphic sites in serotonin transporter protein gene attracted much interest. These are: the variable number of tandem repeats (VNTR) and 5'-flanking promoter region (5-HTTLPR). Keywords: 5-flanking promoter region, chronic tension-type headache, haplotypes, serotonin transporter protein gene, a variable number of tandem repeats Primary headaches constitute a major health problem and this is why there has been an increasing interest in the genetic associations of these widespread disorders within the last couple of years. Chronic tension-type headache (CTTH) occurs on at least 15 days in a month for up to three months and requires a visit to the family practitioner, neurologists and other physicians. [1] A recent study has shown that CTTH is one of the most serious reasons for the loss of productive effort. [2] A Danish study showed that 12% of employed subjects with CTTH had missed one or more days of work in a given year because of headache. The total loss of workdays per year due to tension-type headache in the general population was estimated to be 820 days in 1000 persons. [3] Studies in Turkey showed that CTTH had a higher impact on loss of productivity and drug costs, going on to have a larger economic impact. [4] In order to address the role of the serotonergic system on pathophysiologic mechanisms of CTTH, some studies have been published about one of the key modulators: serotonin transporter protein. [5],[6],[7] Serotonin is uptaken from the synaptic space regularly with a 5-hydroxytryptamine transporter (5-HTT) and returned to the neurotransmitter pole to be used again in succession. [8],[9] Serotonin transporter protein (5-HTT) is encoded by the single gene SLC6A4 on Chromosome 17q12. [10] Two polymorphic sites in 5-HTT gene grabbed interest: a variable number of tandem repeats (VNRT) of 17-bp repeats in intron two as it has several alleles such as STin 2.7, STin 2.9, STin 2.10, STin 2.11, STin 2.12 and an insertion/deletion in 5¢-flanking promoter region (5-HTT gene-linked polymorphic region-5-HTTLPR) creating a short (S) and a long (L) allele. The 5-HTTLPR polymorphism is situated in a GC-rich region composed of 20-23 bp repeating units. The S and L alleles have 14 and 16 repeat-elements respectively. [11],[12] The short form of this variant, "S" is associated with lower basal and induced transcriptional efficiency of the 5-HTT gene promoter, resulting in lower serotonin uptake activity, when compared with the long form "L". [10] Further studies revealed analogous functional consequences of 5-HTTLPR on 5-HTT expression in brain cells and tissues. [13],[14] Some studies indicate that the 12-repeat allele is associated with higher enhancer-like properties for the transcription of the 5-HTT gene than 10-repeat allele while other studies have found no associations. [14],[15],[16],[17],[18] There is some evidence to suggest that the 5-HTT gene may be involved in the pathogenesis of migraine with aura and CTTH and both polymorphic regions have been objects for studies. These results support the hypothesis that drugs primarily acting via 5-HTT inhibition, such as SSRIs and serotonin agonists may be effective in the pharmacotheraphy of headaches. The aim of this study is to investigate the possible role of 5-HTTLPR and VNTR polymorphisms individually and in combination in CTTH patients. Moreover, we aim to evaluate the relationship between the clinical response of the drugs and the serotonin transporter (5-HTT) gene polymorphisms. Materials and Methods One hundred and twenty-six CTTH patients (109 females and 17 males, mean age of 38 ± 18.24 years) and 138 control subjects (117 females and 21 males, mean age of 23.29 ± 6.67 years) were included in this prospective study. The operational diagnostic criteria of the International Headache Society (IHS) were used to evaluate patients with CTTH. [1] Chronic tension-type headache is typically bilateral, pressing or tightening in quality and occurs on ≥15 days/month on an average of ≥3 months, lasting hours or continously. Patients and control groups with episodic migraine or features of nausea, vomiting, photophobia or phonophobia over a period of at least three months were excluded. All participants were interviewed in an outpatient clinic and examined neurologically by a neurologist before being followed for eight weeks. The control group consisted of healthy people having no type of headache or any other disorder. There were no significant differences in the baseline demographics between the study and the control groups. All study subjects signed informed consent before participating in the research. The CTTH and control group subjects were of the same ethnicity, but none were of the same family. The CTTH patients had not used SSRI (serotonin reuptake inhibitors) or amitripytyline and were not drug abusers. The treatment consisted of randomized amitripytyline 10 mg/day or SSRI (citalopram 20 mg/day or sertraline 50 mg/day) but none had placebo. Comparisons between the groups were assessed by visual analogue scale (VAS) for outcome. Control visits were done once a month and in every visit VAS scores were asked. Responders were defined as those with a decrease in VAS by 50% since the beginning. DNA extraction and analysis With a written informed consent, a blood sample was drawn from each individual. The DNA was extracted from the whole blood using a genomic DNA purification kit (MBI Fermentas, Cat:12200, USA). An insertion/deletion polymorphism (5-HTTLPR) in the promoter region of the serotonin transporter gene was typed by PCR using the Lesh et al. , method. [11] A variable number of tandem repeats (VNTR) polymorphism in intron 2 of the 5-HTT gene was typed by PCR using the Cook et al. , method. [19] Genotyping was based upon independent scoring of the results by two reviewers who were unaware of case/control status. Statistical analysis In the analysis of the combination of 5-HTTLPR genotype, the rates of the long (L) and short (S) alleles and 5-HTT gene VNTR genotype 12 and 10 alleles were compared between the CTTH and control groups. [20] The genotypes were compared with the efficacy of the drugs according to the VAS results. χ2 tests, Fischer′s exact test and Kolmogrow Smirnow test were included where applicable. ANOVA was used to evaluate differences in the VAS. SPSS standard software (version 11.0) was used in all analyses and P < 0.05 was considered as significant. Results The observed genotype counts were not deviated significantly from those expected according to the Hardy Weinberg Equilibrium ( P > 0.05) [Table - 1]. The functional polymorphisms of the 5-HTTLPR gene and VNTR were analyzed for all study subjects [Table - 1]. One of the major VNTR alleles, STin 2.9, was present in two patients and was included in the STin 2.10 group. The L allele and the S allele, the 12 allele and the 10 allele with genotype frequencies for both the CTTH and the control groups are presented in [Table - 1]. There were no statistically significant results between each group according to 5-HTTLPR gene alleles, but STin 2.12/12 genotype and STin 2.12 allele predominated in the control group. In order to investigate the combined effect of the two polymorphic loci on the 5-HTT gene expression, samples were separated into nine groups: Genotypes (L/L-12/12), (L/L-12/10), (L/L-10/10), (L/S-12/12), (L/S-12/10), (L/S-10/10), (S/S-12/12), (S/S-12/10), (S/S-10/10). Genotypes (S/S-12/10) and (L/S-12/10) reached statistically significant frequency in the CTTH group than in the control group (χ2 = 5.64 P = 0.017, χ2 = 3.89 P = 0.048 respectively). The combination of genotype frequencies in the CTTH and the control groups are summarized in [Table - 2]. Duration and frequency of headache significantly improved after eight weeks of treatment ( P < 0.001). No significant difference was noticed between 5-HTTLPR and VNTR genotype groups and success in treatment due to 50% decrement in VAS scores ( P = 0.996). There were no significant differences between genotypes and severity of CTTH (VAS ≥ 7) either ( P = 0.784). There was no difference between drugs and response to treatment (χ2 = 0.22, P = 0.636).Discussion Tension-type headache studies have not been conducted as much as migraine studies. Recently, the ICHD-II (The international classification of headache disorders) revised the criteria incorporating many developments and presented an effective classification. [1] In comparison to the general population, first degree relatives of CTTH patients had three times more risk of CTTH. This result supports the importance of genetic factors in CTTH. [21] Epidemiological studies on tension-type headache frequency and genetic polymorphisms may lighten the risk factor of 5-HTT gene polymorphism. The presence of S allele has been found to have less serotonin activity and serotonin uptake. [7],[11],[12] In Chinese and Korean study groups, S allele has been found two or three times more frequently than L allele and depressed patients with L allele showed better response to SSRIs. [18],[22],[23] Two studies from the same population showed no significant association between migraine frequency and S allele, but demonstrated a difference in the genotype distribution of S allele in patients with CTTH. [6],[18] Besides, in the same studies, patients with S allele had significantly more frequent attacks of migraine than those with L allele. [18] The 5-HTTLPR S allele has been associated with slower response to various antidepressant treatments [24],[25],[26],[27] though not univocally. [28] There are controversial results with association of S allele and migraine. [29],[30] According to our results, genotypes are not observed in association with response to SSRIs and TCAs. In our study, S allele was more frequent both in the CTTH and control groups (56%, 55% respectively), but not as much as the frequency of the Korean people with S allele at the rate of 86%. [19] The VNTR polymorphism in native expressing cells showed no significant effect on 5-hydroxyindoleacetic acid level in the cerebrospinal fluid, but revealed a higher level of norepinephrine metabolite in STin 12/12 group. [31] STin 2.12 has been found to be associated with the risk of anxiety disorders and we know that tension-type headache has been seen in combination with anxiety disorders. [32],[33],[34] Another study suggested that migraine patients with or without aura had an over-representation of STin 2.12. [35] Varied results of these polymorphism studies let us think that other factors like enzymes, serotonin receptors and polymorphisms may play a role in the serotonergic system. According to our results, predominance of STin 2.12/12 genotype and STin 2.12 allele in the control group may postulate that susceptibility to CTTH had a genetic component. The association between the VNTR polymorphism and CTTH deserves further evaluation. Although there is no statistical difference between the efficacy of drugs and the genotypes, the benefit on headache duration and severity was significant ( P < 0.05). Clinical response to SSRIs and TCAs may indicate the serotonergic dysfunction in the central nervous system of the CTTH patients. Independence of the efficacy of drugs from the genotypes means that studying a single factor involved in serotonergic activity may not be enough to end up this subject. An increased knowledge of the genetic risk factors will give an opportunity to understand the pathogenesis of CTTH, which is therefore expected to enable clinicians to select people who will have a high risk of CCTH and benefit from treatment. As mentioned above, all of the studies were aimed at looking into the effect of a single polymorphism of 5-HTT function separately. However, it is much more informative to analyze markers in a region of interest simultaneously. Genotype analysis should be tested in large clinical samples in order to increase knowledge about CTTH susceptibility. It is also possible that the heterogeneity among diseases showing the same clinical research will require time and effort for individual identification. Although these two polymorphisms have been investigated individually and extensively for association with migraine and psychological symptoms, to our knowledge, there are no reported studies on the combined effect of 5-HTTLPR and VNTR genotypes on CTTH. According to our results, we may suggest that the presence of one/two S allele(s) with STin 2.12/10 may be responsible for having CTTH. Furthermore, the results revealed that the homozygous S group with STin 2.12/10 was more significant with P = 0.017 than the heterozygous S group with STin 2.12/10. At this point, we may be able to make reliable comparisons and hypotheses on the homozygous and/or the heterozygous presence of S and STin10 alleles; and their possible interaction with the CTTH. In L/L-10/10 group, the results may indicate that the present homozygous STin 2.10 allele does not act as a dominant allele in combined effect ( P = 0.08). However, STin 12/10 genotype may be in interaction with the S allele in CTTH patients. This datum supports that the action of genetic variation at the VNTR locus is influenced by other genetic and environmental influences. On the other hand, the presence of homozygous L and STin12 alleles may play a protective role against CTTH. Recently, a new possible combined effect of alleles on 5-HTT expression is indicated as low-expressing (short [S], 10); but high-expressing (long [L], 12) in schizophrenics. VNTR polymorphism 10 allele has acted as the dominant low-expressing allele in genotypes and reduced relative 5-HTT gene expression on lymphoblast. [36] In our results, combined genotypes S/S-12/10 and L/S-12/10 had significant interaction with the CTTH group. Guidelines for complex diseases recommend that 500 samples for patients and controls will give sufficient results. Larger study groups will give more reliable results. In this study the CTTH is compared with healthy subjects. Another study dealing with the comparison of chronic headache with non-chronic headache or other chronic illnesses may be a better way. Another limitation of this study is that the anxiety and depression traits were not screened and we could not analyze them with genotypes. In conclusion, to our knowledge, this is the first study resulting with modest evidence for a possible combination of the 5-HTTLPR and VNTR polymorphisms with CTTH. Further large, cross-ethnic studies including psychiatric assessment are needed to determine whether alterations in serotonin gene expression are involved in CTTH. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08043t1.jpg] [ni08043t2.jpg] |
| |||||||||

{kind=link}
{kind=link}