 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
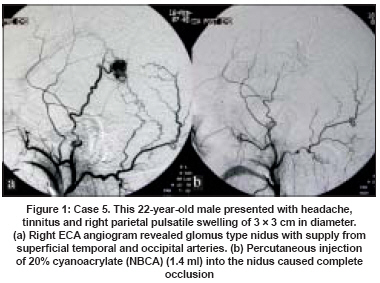
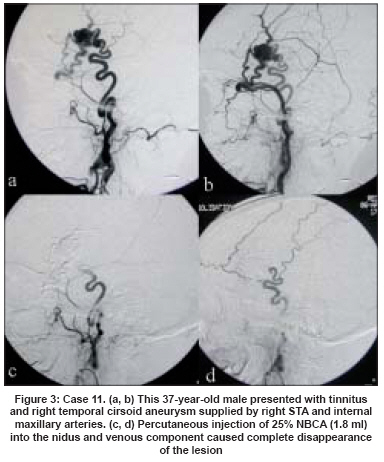
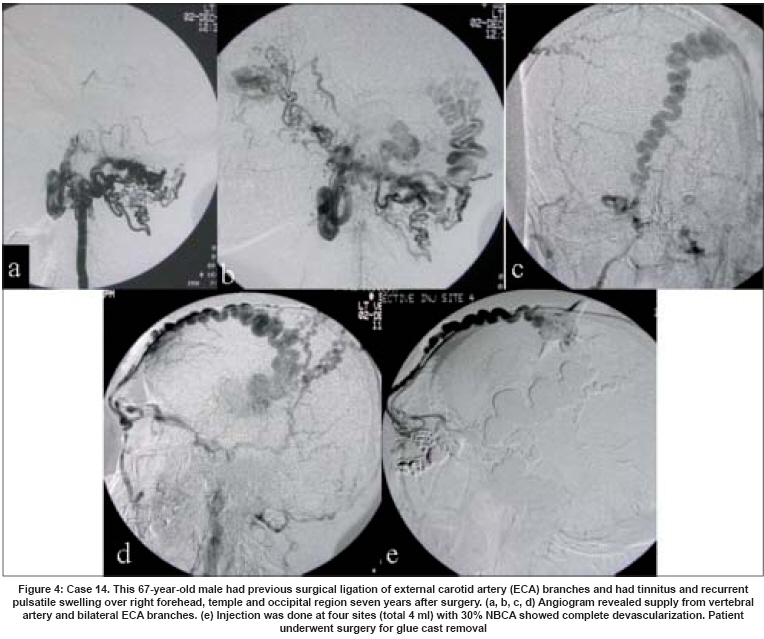
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 167-172 Original Article Endovascular treatment of scalp cirsoid aneurysms Gupta AK, Purkayastha S, Bodhey NK, Kapilamoorthy TR, Krishnamoorthy T, Kesavadas C, Thomas B Department of Imaging Sciences and Interventional Radiology, Sree Chitra Tirunal Institute of Medical Sciences and Technology, Trivandrum, Kerala Code Number: ni08045 Abstract Background: Scalp is the most common site of soft tissue arteriovenous fistulae and surgical excision has been the primary mode of treatment. Endovascular treatment has evolved as an alternative to the surgery.Aims: To evaluate the effectiveness of percutaneous direct-puncture embolization of cirsoid aneurysms. Materials and Methods: From January 1995 to December 2004, 15 patients underwent percutaneous direct-puncture embolization of cirsoid aneurysms. Plain X-ray, computerized tomography scan and complete selective cerebral angiogram were done in all. Seven patients had forehead lesions, four had temporal and the remaining four patients had occipital region cirsoid aneurysms. Lesions were punctured with 21-gauge needle and embolized with 20-50% cyanoacrylate-lipiodol mixture. Circumferential compression was applied during injection. Results: Post-embolization angiogram showed complete obliteration in 11 patients. The remaining four patients required adjunctive transarterial embolization with polyvinyl alcohol particles for complete lesion devascularization. Two patients had post procedure surgery for removal of disfiguring and hard glue cast. There were no major procedure-related complications. No patients had any recurrence in the follow-up. Conclusion: Percutaneous direct puncture embolization of cirsoid aneurysms is a safe and effective procedure. It can be effectively used as an alternative to surgery. Sometimes adjunctive transarterial embolization is also required to deal with deeper feeders. Keywords: Angiogram, cirsoid aneurysms, embolization, percutaneous direct puncture Arteriovenous fistulae were first described by Hunter in 1757. [1] The term cirsoid aneurysm was applied to vascular malformations of the scalp in 1833 by Brecht. [1] The malformation is drained by enlarged, tortuous veins, which may, in parts, show variceal dilatation. Various names have been used to describe these lesions like aneurysma cirsoide, aneurysma serpentinum, aneurysma racemosum, plexiform angioma, arteriovenous fistula, arteriovenous aneurysm and arteriovenous malformation. [2],[3] With the development of endovascular obliteration of the malformation, there has been renewed interest in these lesions. [4],[5],[6],[7] The purpose of this study is to describe our experience with embolization of cirsoid aneurysms in 15 patients. Materials and Methods Clinical details of the patients treated between January 1992 and December 2004 were collected. Fifteen consecutive patients (nine male and six female patients; age range, 7-59 years) with scalp cirsoid aneurysms were treated with direct puncture and the injection of NBCA (Histoacryl-Blue; Braun, Melsungen, Germany) mixed with iodized oil (Lipiodol; Laboratoire Guerbet, Roissy, France). Transarterial embolization was also done as an adjunct to direct puncture embolization in few of them. Our institutional review board approved the procedure. Informed consent was obtained from each patient. All 15 patients presented with pulsatile scalp mass. Four patients (three with parietal and one with an occipital scalp lesion) had local bleeding from the lesion. Nine patients complained of tinnitus, seven patients had focal headache. On examination, in all patients, obvious, pulsatile swellings of the scalp, with dilated vessels leading into the lesion and an audible bruit on auscultation, were encountered. Seven patients had forehead lesions in the frontoparietal region and four of them had an associated temporal region swelling. Four patients had isolated temporal region pulsatile swelling and in four patients the lesion was confined to the occipital region only. The size varied from 2 x 2 to 6 x 6 cm. Compression of the ipsilateral carotid or the main feeding vessel caused the lesion to decrease in size and diminished the bruit. In three patients, lesions involving the forehead region were thought to be traumatic in origin, with a history of head trauma five to seven years ago. In the other 12 patients, the lesions were spontaneous or congenital. Three patients had previously undergone partial excision of their lesion and/or ligation of the feeding arteries. In all these patients, a collateral arterial supply to the lesion had subsequently been recruited. The lesions were supplied by the contralateral external carotid arteries via collateral vessels. Plain X-ray and CT scan of head in all patients showed soft tissue scalp swelling, no intracranial lesion was demonstrated. All patients underwent complete cerebral angiography with bilateral selective internal and external carotid injections to document the location, size, feeding arteries and venous drainage of the lesions. The forehead lesions in seven patients were supplied by combinations of superficial temporal, internal maxillary artery and middle meningeal arteries. Two of them had associated supply from facial artery and twigs from ophthalmic arteries. Temporal region lesions were supplied by superficial temporal arteries, middle meningeal artery and deep temporal arteries. The occipital scalp lesions were supplied bilaterally by the occipital arteries. Posterior auricular arteries also supplied in a few of them. In two patients bilateral vertebral angiography demonstrated opacification of the lesions through direct supply and communication with the occipital artery. In all patients, multiple sites of arteriovenous communication were identified at selective angiography and in no case a single-hole fistula was seen. No intracranial arteriovenous malformation was observed in any patient. Technique of embolization Direct-puncture embolization Procedure was performed under local anesthesia. After selective transarterial angiography, the lesions were punctured in the area nearest to the arteriovenous connection and direct angiography was performed with and without manual compression of the venous drainage in the region. In patients in whom a glomus-like nidus was visualized at angiography, this area of arteriovenous connection was punctured [Figure - 1]. In patients in whom the lesion was extensive and the venous channels were engorged, the venous channel adjacent to the nidus was punctured and embolized [Figure - 2] and [Figure - 3]. To achieve circumferential flow reduction around the lesion, we used a sterilized rounded or oval-shaped metallic ring held in place over the dilated collecting vein with rubber bands. The lesion was punctured by using a 21-gauge butterfly needle. Contrast material injected through this needle showed no distal escape beyond the edge of the metallic ring, indicating adequate venous compression. When more pressure was applied to the metallic ring, the arterial inflow could also be reduced, thereby achieving complete flow reduction in the desired area. With the ring held in place, cyanoacrylate-lipiodol mixture was injected into the nidus or the collecting vein. The metallic ring was left in place for a few minutes and then removed gradually. The operators′ hands compressed the frontal and angular veins in a few cases where the compression by the metallic ring was not possible. The concentration of the NBCA-iodized oil mixture was adjusted according to the flow rate as evaluated at angiography and the injection rate and volume were controlled by using fluoroscopic road mapping during NBCA injections. Repeated puncture and injections were performed when residual lesion was demonstrated at post-embolization angiography or in large lesions [Figure - 4]. Transarterial embolization This was performed as an adjunct to direct puncture when the supply from deeper arteries was seen in the lesions. Transarterial embolization using polyvinyl alcohol particles, gelfoam soaked in alcohol and NBCA was performed for supply from middle meningeal artery, internal maxillary artery, deep temporal artery and posterior auricular arteries. Experienced interventional radiologists were involved in the procedures, retrieval of data and image analysis. Post-procedure assessments were done on the next day of the procedure, at one month and then every six-monthly. All the patients were clinically examined to detect any recurrent swelling, audible bruit etc. Follow-up angiograms were not considered until there was clinical suspicion of recurrence. Results Post-embolization angiograms showed that in 11 patients the lesion had completely disappeared after single or multiple percutaneous injections. Two to six percutaneous injections were needed for complete obliteration. Total volume of cyanoacrylate injected ranged from 1.2 to 6 ml. After cyanoacrylate injection in two patients with a forehead lesion, the blood supply to the lesions from the ophthalmic arteries ceased completely. In four patients, the lesion was more than 90% devascularized. The first two were involved in the forehead as well as temporal region lesions and the last two arteries in occipital lesions. The feeders were identified and embolized transarterially with polyvinyl alcohol particles of 250-355 m size, gelfoam soaked in alcohol and NBCA. Total reduction of blush was achieved. After percutaneous embolization, in two patients lesions were resected due to cosmetic reasons. Immediately after injection, thrombosis occurred in the lesions, which became swollen and hard. After embolization, most patients reported pain at the injection site. This pain, due to the glue injection, was managed effectively with intravenous administration of analgesics. In one patient with large occipital scalp lesion, a small amount of glue drained out of the lesion to the external jugular vein during injection. But it was clinically silent. There was no other procedure-related complication or delayed skin problems. We have six months to 11 years follow-up in 13 patients. No patient had any recurrence of pain, swelling or tinnitus. There was no audible bruit in them. So there was no clinical suspicion of any recurrence and angiogram was not repeated in them. Discussion A cirsoid aneurysm of the scalp is an abnormal fistulous connection between the feeding arteries and draining veins, without an intervening capillary bed. [8] Soft tissue arteriovenous fistulae occur most commonly in the scalp. Although only 14% of the body surface area is in the head, 50% of the integument arteriovenous fistulae occur in this region. [9] When these abnormal fistulae enlarge to a size that is clinically recognizable and there are large, dilated draining veins, the lesions are termed cirsoid aneurysms. [10] Most congenital lesions become symptomatic in the third decade of life (range, three months to 59 years of age). Sixty per cent of the affected persons are male. The location of scalp cirsoid aneurysms is roughly evenly distributed among the frontal, temporal and parietal regions. [2] Although controversy still exists regarding the cause of these lesions, it is generally accepted that they may be either of congenital or traumatic origin. In our series, 20% of the lesions could be directly related to trauma (blunt, non-penetrating trauma in the majority). Penetrating trauma as a cause is well described, including iatrogenic-induced fistulae after hair transplantation, arthroscopy of the temporomandibular joint and craniotomy for intracranial procedures. [11],[12],[13],[14],[15],[16],[17] Congenital malformations are more frequent and constituted 80% in our series. Theories about their occurrence include persistence of primitive arteriovenous fistulae. [18] Familial scalp fistulae are extremely rare. [2],[3] Almost all patients present with a scalp swelling that has gradually increased in size from birth or after head trauma. Rapid increases in size have been reported to occur at puberty, during menstruation and during pregnancy. [19] Associated symptoms and signs include pain, throbbing headaches and bruits. [19] Hemorrhage from the lesion is uncommon. [20] Large lesions have also been associated with scalp necrosis. [20] Vascular endothelial growth factor is expressed by these lesions and is responsible for their continuous growth. [21] Rarely, they can present with epilepsy. [22] The diagnosis is clinical in the majority of patients. Angiography is undertaken to delineate the lesion and to exclude an intracranial component. [23] This takes the form of an enlarged middle meningeal artery with fine feeding vessels running through the bone feeding the malformation. [3] Yokouchi et al . classified scalp arteriovenous fistulae into three types: Type A: has a single fistulous connection from the proximal portion of the artery, Type B: has a single fistulous connection but from multiple distal portions of the arteries and Type C: where there are multiple fistulae constituting the plexiform feeding type. [24] Sometimes the drainage can be intracranial with an associated cerebral arteriovenous malformation. [25] The diagnosis of scalp cirsoid aneurysm and its differentiation from sinus pericranii can be difficult and some confusion between the two types of lesions exists in the literature. Strictly speaking, sinus pericranii is a collection of non-muscular venous blood vessels tightly adhering to the outer surface of the cranium and communicating directly with a intracranial venous sinus via deploic veins. [25],[26] Indications for treatment are the prevention of hemorrhage, tinnitus and the cosmetic relief of the pulsatile swelling. Treatment options include surgical excision, ligation of the feeding vessels, transarterial and transvenous embolization, injection of sclerosant into the nidus and electrothrombosis. [4],[5],[6],[7],[27],[28],[29],[30],[31],[32] In the past, treatment of arteriovenous malformation of the scalp and face was primarily reliant on surgical excision or ligation of the feeding arteries. [26],[27],[28],[29],[30],[33] Some lesions were so large that excision was not possible. [34] Ligation of feeding arteries has been particularly troublesome because of the recruitment of a collateral vessel supply and the loss of access to the fistula for further embolization. [35] Transarterial and transvenous embolization of scalp cirsoid aneurysms has been used as an adjunct to surgery or as definitive therapy. [35],[36] Embolization alone could remedy a scalp arteriovenous fistula and improve the grotesque feature without scalp ischemia. [4],[6] In cases of a cirsoid aneurysm of the scalp, direct-puncture embolization with NBCA, absolute alcohol or a metallic thrombogenic coil has been reported. [37],[38] In direct-puncture embolization, the targeted vessel is the venous structure just distal to the arteriovenous connection. Occlusion of the vascular structures with this technique thus involves no risk of ischemic skin complications. Immediate venous occlusion allows continuous redistribution of the embolic agent to adjacent vascular spaces and effective devascularization occurs without complications. During treatment with NBCA embolization by means of direct puncture in the 15 consecutive patients in our series, there were no complications involving puncture of the lesion, occlusion of venous channels or abrupt occlusion and thrombosis of the nidus. For temporary occlusion of the venous outflow, elastic ring, elastic strap, a ring-shaped compression device can be used, thus avoiding exposure of the operator′s hand to radiation. In this series, multiple direct-puncture angiographies were followed by adjustment of compression points and venous channels were thus completely occluded. We are using this technique since 1995. Recently Duncan et al . described it as ′cookie-cutter technique.′ [39] In most lesions, a large, high-flow arteriovenous fistula often is associated with the aneurysm and the embolus must, therefore, be large; otherwise, the embolus may pass into the pulmonary circulation. Temporary manual compression of the venous drainage during NBCA injection slows down the blood flow and can prevent inadvertent washout into the distal venous outflow tract and pulmonary circulation. We have not encountered any pulmonary embolism related to the procedure. Lodging of embolic materials like coils in proximal feeding vessels lessens the blood supply and has been a helpful adjunct to surgery but rarely is curative. [4],[6] Recent developments in the design of microcatheters and distal navigation techniques have made possible the catheterization of feeding arteries close to the nidus. Injection of NBCA with a microcatheter wedged into the nidus may lead to permanent devascularization of an arteriovenous malformation without risk of ischemia of the adjacent normal tissue. But total devascularization involving transarterial embolization of the multiple feeding arteries may, however, be ineffective or technically difficult. So transarterial route of embolization can only be used as an adjunct to direct-puncture embolization of cirsoid aneurysms. Conclusion Percutaneous direct-puncture embolization of cirsoid aneurysms is a safe and effective procedure. It can be effectively used as an alternative or adjunct to surgery. Sometimes adjunctive transarterial embolization is also required to deal with deeper feeders.References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08045f3.jpg] [ni08045f4.jpg] [ni08045f1.jpg] [ni08045f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}