 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
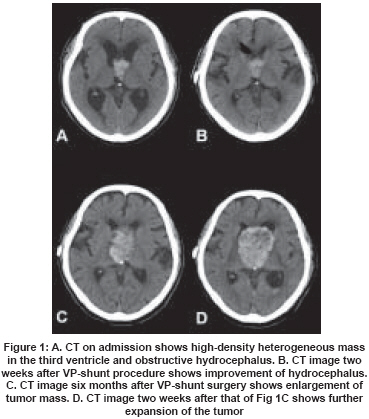
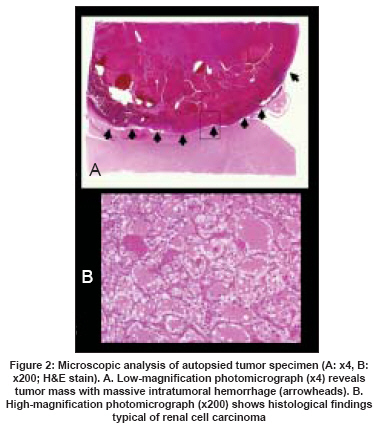
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 179-181 Case Report Solitary metastasis of renal cell carcinoma to the third ventricular choroid plexus with rapid clinical manifestation by intratumoral hemorrhage Tomiyama Arata, Nakayama Haruo, Aoki Kazuya, Ueda Morikazu 2nd Department of Neurosurgery, Toho University Ohashi Medical Center, Tokyo Code Number: ni08047 Abstract A 72-year-old man who had undergone nephrectomy for left renal cell carcinoma (RCC) presented with worsening of cognitive function and frequent loss of consciousness. Computed tomography (CT) revealed tumor mass in the third ventricle and hydrocephalus. A ventriculoperitoneal (VP) shunt was placed to treat the hydrocephalus. The postoperative course was uneventful, and he was followed closely without aggressive therapy. Four months after surgery, the tumor expanded rapidly due to intratumoral hemorrhage and he died due to sepsis. The autopsy findings revealed a solitary metastatic RCC in the third ventricle, with massive intratumoral hemorrhage. Solitary metastasis of RCC to the third ventricle is quite rare and difficult to treat. The case report highlights that early diagnosis and treatment are critical, even in slowly progressive RCC patients, because of the possibility of intratumoral hemorrhage.Keywords: Brain metastasis, renal cell carcinoma, third ventricular choroid plexus Although the choroid plexus receives an abundant supply of blood, metastasis of renal cell carcinoma (RCC) to the choroid plexus is the least common form of brain metastasis. [1],[2],[3] In particular, a metastasis to the third ventricle has never been reported. We describe the first case of a solitary metastasis of RCC to the third ventricle, which resulted in acute clinical symptoms due to recurrent intratumoral hemorrhages, and discussed with an emphasis on therapeutic aspects. Case Report A 72-year-old man was admitted to our hospital in August 2003 because of progressive worsening of cognitive function. Sixty months ago, the patient had a medical history of RCC treated with left nephrectomy followed by irradiation (50 Gy) and oral 5-FU (Fluorouracil) treatment. The patient appeared drowsy upon neurological examination at the time of admission (Glasgow coma scale (GCS) E3V4M5). The computed tomography (CT) scan of the brain showed a high-density mass in the third ventricle, without contrast medium, and hydrocephalus [Figure 1A]. Emergency VP shunt operation for the hydrocephalus was performed, and the patient′s symptoms improved. Cerebral CT scan after surgery showed improvement of the hydrocephalus [Figure 1B]. And, after considering next strategy of therapy, we finally elected to closely monitor the patient without therapy including Gamma knife surgery (GKS), in consideration of the patient′s general health, poor neurological status (Karnovsky performance status (KPS)=30~40), age, tumor location , and family desire. However, in January 2004, the patient′s consciousness level suddenly deteriorated, and emergency cerebral CT revealed sudden enlargement of the tumor [Figure 1C]; additional head CT study two weeks later showed that the volume of the tumor had increased by up to 6 cm in diameter due to recurrent intratumoral hemorrhage [Figure 1D]. Administration of steroids and osmotic diuresis drug was started, but the patient′s level of consciousness began to worsen further as tumor size increased. Finally, six months after surgery, he died from sepsis. The autopsy findings revealed a solitary tumor in the third ventricle that had originated from the choroid plexus. The tumor was filled with hematoma [Figure 2A], and the tumor histopathology resembled that of RCC [Figure 2B]. Discussion Metastasis of RCC to the brain occurs in about 10% of RCC patients. [4] Within these cases, solitary choroid plexus metastasis of RCC is very rare, with only 10 cases, including our case, reported in the literature. [1],[2],[3] A choroid plexus metastasis in the third ventricle is thought to be a subtype of choroid plexus metastasis in the lateral ventricle, because of the anatomic continuity; however, there is no report of solitary metastasis to the third ventricle. It is well known that the postoperative course of RCC varies considerably, and RCC is usually classified as rapidly or slowly progressive. [3],[5] In the present case, 60 months elapsed from the diagnosis of RCC until detection of the intraventricular tumor, with no evidence of biochemical abnormality. Thus, our case was slowly progressive RCC. However, intratumoral hemorrhage occurred repeatedly in the last six months and the patient′s clinical symptoms deteriorated rapidly. The therapy of choice for metastatic RCC is surgical resection plus irradiation or irradiation alone (including GKS). Wronski et al. , studied 50 cases of surgical resection plus entire brain irradiation and found that median survival was 12.6 months. [6] Hoshi et al., investigated 42 cases with metastasis of RCC to the brain that were treated only with GKS plus entire brain irradiation and found that the median survival was 12 months. [7] However, GKS plus entire brain irradiation had a superior local control rate of 93% and management mortality rate of 4.7%. [5] The efficacy of chemotherapy and immunotherapy for intracranial metastasis of RCC has not been proven. [8] In addition, one report suggested that Interferon (INF)-alpha during RCC treatment may be even neurotoxic. [9] Although one case has been reported in which an intracranial lesion disappeared after only long-term oral administration of 5-FU, [10] these findings had no bearing on our case. When considering treatment of metastases of RCC to the intraventricular choroid plexus from a general anatomic perspective, surgery and radiation therapy are both indicated for intralateral ventricular metastases. However, when the tumor metastasizes to the third ventricular choroid plexus, as in the present case, both treatments must be considered carefully because of the risks of damage to peripheral structures and bleeding from tumor. [3] In addition, intraventricular metastases can grow larger, without clinical symptoms. From this perspective, the indications for surgical resection and irradiation therapy may also be restricted. However, when treatment is not conducted at an early stage, tumor volume-even in slowly progressive RCC-may increase rapidly due to recurrent intratumoral bleeding, which can cause progressive neurological deterioration, due to hypothalamic damage or impairment of the hypothalamus. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08047f2.jpg] [ni08047f1.jpg] |
| |||||||||

{kind=link}
{kind=link}