 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
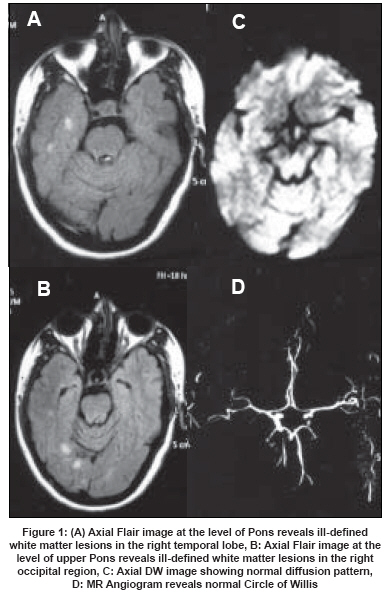
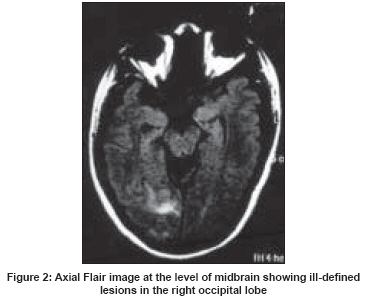
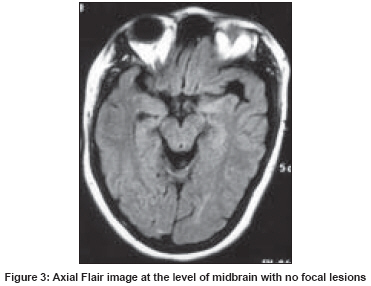
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 182-185 Case Report Reversible white matter abnormalities in a patient with migraine Agarwal Shalini, Magu Sarta, Kamal Kirti Department of Radiodiagnosis, Pt. B.D. Sharma, PGIMS, Rohtak, Haryana - 124 001 Code Number: ni08048 Abstract A 35-year-old female with migraine without aura, presented with sudden onset of visual aura along with loss of vision on the left side. Following this she had nausea, vomiting and headache. Magnetic Resonance Imaging (MRI) performed at this stage revealed ill-defined lesions hyperintense on Flair images, located in the right temporal and right occipital region. Diffusion weighted images, MR angiogram, T1-weighted and T2-weighted images were normal. She got relief with symptomatic treatment. Twenty days after this attack of migrainous aura she had a similar episode. An MRI scan was performed again. It revealed similar lesions only in the right occipital lobe. Follow-up MRI performed seven weeks later was normal.Keywords: Ischemia, migraine, magnetic resonance imaging Migraine is a very common debilitating disorder. Patients with migraine are at increased risk of white matter hyperintensities detected on magnetic resonance imaging (MRI). Also, migraine has been implicated as an independent risk factor in stroke with the incidence of active migraine (both with an without aura) in stroke patients as high as 3.7%. [1] These nonspecific white matter hyperintensities may cause uncertainty for the physicians and anxiety for patients. [2] The relationship between migraine and silent white matter changes is controversial. There are no postmortem studies identifying the pathology of these MRI characteristics and their true etiology is unknown. [3] We present a case of migraine with typical aura who presented similar, but reversible white matter abnormalities in the posterior cerebral artery territory. Case Report A 35-year-old female doctor presented with complaints of headache off and on for the past 20 years. These were only occasionally associated with nausea and vomiting. These were aggravated by light (including sunlight, Halogen lights and play of colors) and relieved by sleeping and over-the-counter analgesics. The frequency was two to three mild headaches/month and one to two severe headaches/ month. The severity has been rated according to her ability to carry out routine daily activities. These headaches were mainly localized in the frontal region and were pulsating in quality. These lasted for approximately 4-6 h. These attacks of headache were associated with photophobia and phonophobia. The duration and frequency of headaches gradually increased over the years. There was history of multiple corrective surgeries for congenital squint and family history of father suffering from similar headaches till 20 years of age. These were, however, not associated with aura. The findings were consistent with migraine without aura (1.1 of ICHD-II).There was no history of analgesic overuse. There was no history of cerebrovascular or thromboembolic disease, diabetes or miscarriage. There was no history of childhood periodic syndromes. On 20 August 2007, for the first time, the patient experienced aura in the form of flashes in the sky along with loss of vision in the left half of the field. There were no associated sensory, motor or language symptoms. The aura lasted for approximately 20 min. The flashes were followed by scotomas with bright shimmering borders in that particular area of visual fields . Aura was followed by nausea, vomiting and headache for which she took injection metoclopromide intramuscularly and an over-the-counter analgesic. She was fine after getting up from sleep in the morning. Next day she again experienced similar kind of aura which again lasted for approximately 20 min. This was followed by projectile vomiting and headache which lasted the whole day. She was put on prophylactic treatment with Tab Flunarazine 10 mg (1 tab at night). An MRI was performed on the next day which revealed multiple ill-defined white matter hyperintense lesions on Flair images [Figure 1A, B] in the right temporal and right occipital region. Rest of the sequences including T1-weighted, T2-weighted and diffusion-weighted images were normal. [Figure 1C]. An MR angiogram was also normal. [Figure 1D]. One week later she again had aura in the form of flashes of light which was followed by mild headache and desire to avoid light. She took Tab Domset (combination of Domperidon and Paracetamol) for symptomatic relief in addition to Tab Flunarazine prophylaxis. Twenty days following the earlier attack of migraine with aura the patient experienced another episode of headache which was preceded by aura in the form of silver-colored flash in the left upper quadrant of her visual field and loss of vision of left half of visual field which lasted for approximately 15 min. This was followed by dizziness and headache which persisted off and on for 11/2 months. There was no associated nausea and vomiting. The MRI performed at this stage revealed total resolution of the lesions seen in the previous MRI performed 20 days earlier, instead there were similar lesions in the right occipital region seen on Flair images [Figure - 2] with normal T1-weighted, T2-weighted and diffusion-weighted images. The MR angiogram was also normal. Single Photon Emission Computed Tomogram (SPECT) was performed on the next day using intravenous administration of Technetium-99m ethyl cysteinate dimer (99m-Tc ECD) and it revealed mild hypoactivity in bilateral high medial frontal cortices. Various hematological investigations performed at this stage revealed mildly raised triglyceride levels. Three days later she was put on Tab Propranolol prophylaxis 20 mg twice a day in addition to Tab Flunarazine. The aura, in the form of silver-colored flash, persisted off and on for approximately 10 days. The size of the flash and the frequency of aura gradually reduced. All the medicines were stopped after three months. Since then the frequency of headaches is again gradually increasing. Various investigations to rule out other causes of headache and stroke in the young were within normal limits. Systemic examination including complete neurological examination and cardiovascular examination was within normal limits. Features during the study period are consistent with migraine with aura (1.2 of ICHD-II). An MRI performed seven weeks after the second episode of migrainous aura was normal [Figure - 3]. Discussion Migraine is a frequently unilateral and throbbing form of headache occurring in paroxysms associated with neurological, gastrointestinal, and autonomic symptoms. Although its prevalence varies from country to country, it occurs in 5 to 20% of the population. More than half of the patients are female, and the female to male ratio varies from 3:2 to 3:1. Migraine usually presents itself in the third decade of life. In 25% of patients, however, it emerges after 40 years of age. There is a family history of migraine in 45 to 80%. [4] In 20% of cases the migraine headache is preceded by visual hallucination/ illusion known as aura. [5] Cerebral Abnormalities in Migraine, an Epidemiological risk analysis (CAMERA) study by Kruit et al., [6] described a specific pattern of small cerebellar infarct-like lesions in migraine patients, notably in those with aura. They concluded that a combination of (possibly migraine-related) hypoperfusion and embolism is the likeliest etiological mechanism. Meta-analysis performed by Swartz et al , [7] showed that there is a strong relationship between migraine and MRI white matter abnormalities (WMA), regardless of comorbidities. Individuals with migraine are close to four times more likely to show these changes than age- and sex-matched controls. This applies even to studies of young (55 years old) people with no other identified risk factors beyond migraine. These lesions have been best described on T2-weighted or FLAIR sequences on MRI, in the deep or periventricular white matter. [8] Diffusion and perfusion-weighted studies have been reported as normal. These usually occur in the territories of the posterior or middle cerebral arteries. [9] However, Demirkaya et al. , [10] reported bilateral anterior cerebral artery territory infarction. The MR angiography was normal. In our case report, the ill-defined white matter lesions were seen only on Flair images in the territory of the posterior cerebral artery. These were reversible and correlated well with the clinical condition. Liang et al, [11] reported a case of migrainous infarction with appearance of laminar necrosis. On review of the literature they could find a report of only one other such case. Computed Tomogram (CT) angiogram and MR angiogram were normal. Cortical spreading depression (CSD) theory was further corroborated by a study performed by Hadjikhani et al., [13] who observed blood oxygen level-dependent (BOLD) signal changes that demonstrated at least eight characteristics of CSD, time locked to percept/ onset of aura using high-field functional MRI with near continuous recording during visual aura in three subjects. Rozen TD [3] described a patient with migraine who developed right cerebellar hemisphere infarcts which disappeared on repeat imaging 16 days later, questioning their etiology as vascular ischemic-based infarcts. The findings in our patient were very similar. Lizuka et al., [14] reported a patient with sporadic hemiplegic migraine who provided several important clues to the mechanism of persistent aura. First, focal hyperperfusion was seen in the brain regions corresponding to persistent aura symptoms. Second, augmented vasogenic leakage in the most affected posterior brain was demonstrated on delayed enhanced FLAIR image. Third, these focal cerebrovascular changes completely resolved when persistent aura symptoms disappeared following corticosteroid therapy. These observations suggested that an uncoupling hyperaemia might exist in the brain regions corresponding to persistent aura of hemiplegic migraine. Positron emission tomography (PET) and MRI studies have shown functional abnormalities in the brainstem (in particular in dorsal Pons) in migraine patients during an attack and in patients with chronic migraine. [15],[16] These abnormalities suggest the possibility of structural changes. In patients of hemiplegic migraine cerebral edema, glucose hypometabolism, and cerebral hyper- and hypoperfusion have previously been reported using PET and SPECT scans. Dodick et al. , [17] reported severely reduced glucose metabolism and perfusion involving the entire left hemisphere found on Fluoro-deoxy glucose (FDG)-PET and SPECT scan three months and two years after an episode of hemiplegic migraine in a 43-year-old male patient. In contrast, the results of SPECT study performed in our patient revealed hypoactivity in bilateral high medial frontal cortex. Rocca et al., [18] found that structural gray matter (GM) abnormalities can be detected in migraine patients with brain T2-visible lesions using Voxel Based Morphometry (VBM) and a high-field MRI scanner. Such GM changes comprise areas with reduced and increased density and are likely to be related to pathological substrates associated with this disease. Occasionally, white matter lesions in a migraineur may indicate an underlying disease such as cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS), or central nervous system vasculitis. The ability to distinguish between nonspecific and disease-specific patterns of white matter hyperintensities in migraine sufferers is important for the practicing clinician. [2] Findings in our case were unlike the findings in CADASIL and vasculitis, however, findings in MELAS form an important differential diagnosis even though no evidence of any stroke or basal ganglia lesions were observed. Conclusion We present an interesting case of a female patient with history of headaches which can be classified as migraine without aura (1.1 of ICHD-II) which progressed to migraine with aura (1.2 of ICHD-II) and WMA on MRI scan which appeared with each attack of aura and clearly revealed a reversible nature. What this means as far as the pathophysiology of this debilitating condition is considered needs to be evaluated further.References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08048f2.jpg] [ni08048f3.jpg] [ni08048f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}