 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
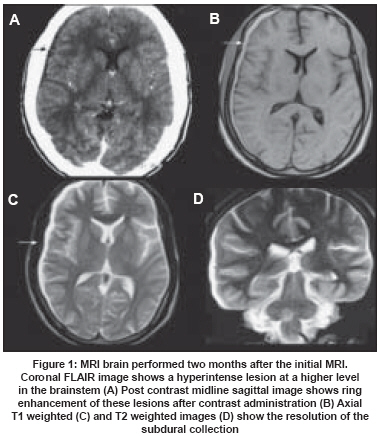
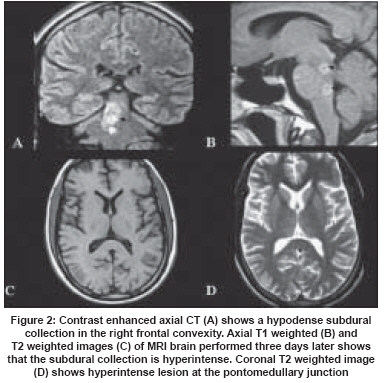
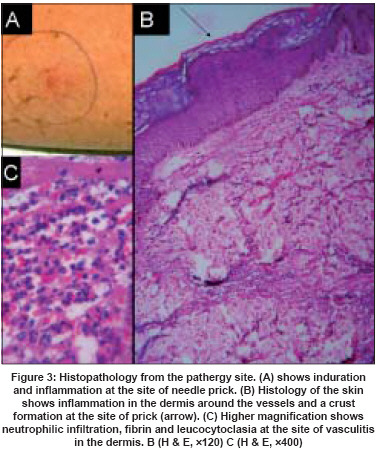
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 195-197 Case Report Acute subdural effusion in vasculitis Raghavendra Seetharam, Kamath Vidya MadavanaVenugopal, Sarada C, Radhakrishnan Ashalatha, Kesavadas Chandrasekharan, Krishnamoorthy Thamburaj Department of Neurology, Sree Chitra Tirunal Institute for Medical Sciences and Technology,Trivandrum, Kerala Code Number: ni08052 Abstract We report a 29-year-old man with a unique presentation of vasculitis as acute unilateral subdural effusion and meningoencephalitis. Magnetic resonance imaging showed a brainstem lesion that spread to the thalamus over time. There were no systemic features of vasculitis other than a positive pathergy test. Histopathological examination from the pathergy site showed neutrophilic infiltrate and leucocytoclastic vasculitis. The condition was steroid responsive and he remained in remission at two years' follow-up. The anatomy of the brainstem lesion, absence of other inflammatory and infective conditions on evaluation suggests a vasculitic pathology either as primary central nervous system angiitis or as neurological presentation of systemic vasculitis like Behηet's disease although the international diagnostic criteria for Behηet's were not fulfilled.Keywords: Pathergy test, subdural effusion, vasculitis Vasculitis affecting the central nervous system (CNS) very rarely presents as acute or chronic meningoencephalitis. [1] Very few cases of subdural effusion in vasculitis are reported in the literature. [2],[3],[4],[5] We report here a case of vasculitis affecting the CNS manifesting as acute unilateral subdural effusion and meningoencephalitis. Case Report A 29-year-old man of Indian origin presented with acute global headache of one-week duration without any signs of raised intracranial tension. He had no significant antecedent medical or neurological illnesses. No history of oral or genital ulcerations or ophthalmic symptoms was forthcoming. There was no history of any recent head injury or trauma. Detailed general physical and neurological examination did not reveal any abnormality. Computed tomography (CT) scan of head revealed a right frontotemporal subdural effusion [Figure 1A]. Over the next three days, he developed ataxia towards the right and bilateral abducens palsy. Magnetic resonace imaging (MRI) brain revealed in addition to the effusion, a right pontomedullary lesion, hyperintense on T2 weighted images (T2WI) [Figure 1B-D]. Magnetic resonance venogram was normal. Cerebrospinal fluid (CSF) examination showed 520 cells/cmm (lymphocytes 80%, polymorphs 20%), protein of 48 mg/dL and normal sugar. Plenty of RBCs was also reported. The CSF gram, fungal and AFB stain, CSF VDRL and CSF TB-PCR were negative. Specific test for Borrelia was not done. All the biochemical investigations, hemogram, ESR, chest X-ray, Mantoux test, serum VDRL, HBsAg, HCV antibodies and HIV-I and II were negative. He was empirically started on a four-drug antitubercular therapy (ATT) (rifampicin 450 mg/day, INH 300 mg/day, pyrazinamide 750 mg/day, ethambutol 800 mg/day) with oral prednisolone 40 mg/day. Patient remained stable clinically; an MRI brain repeated two months later showed new lesions at the mesencephalo-diencephalic junction with extension into the right middle cerebellar peduncle and sparing the red nuclei [Figure 2A]. Lesions showed ring enhancement on contrast study [Figure 2B]. No evidence of earlier subdural effusion was noted [Figure 2C,D]. A repeat CSF study at this stage was normal. His ATT was modified. Pyrazinamide was stopped. Ciprofloxacin 1500 mg/day and ethionamide 250 mg/day were added. He was continued on prednisolone 40 mg daily. Patient gradually showed improvement over the next two months. Six months into the illness, steroids were tapered and stopped, following which his condition worsened to the original status and was referred to our institute. Examination showed, in addition to earlier deficits, patchy sensory impairment over the left upper and lower limbs. A repeat CSF study showed 2 cells/cmm with 100% lymphocytes, normal sugar and mildly elevated proteins (48 mg% and 50 mg% respectively). Serum angiotensin converting enzyme (ACE) assay, serum ANA, APLA, RA factor, LE cell test and serum calcium were normal. A pathergy test was pursued that was positive [Figure 3A]. Skin biopsy from the test site favored the diagnosis of vasculitis [Figure 3B,C]. The ATT was withdrawn. Patient was restarted on higher doses of oral steroids (prednisolone 1 mg/kg/day, 60 mg/day) with which he made a gradual and partial recovery of neurological signs in two weeks. Disabling gait ataxia improved to independent ambulation and scanning dysarthria moderately improved. A marginal improvement in his bilateral sixth nerve palsy was also noted. Sensations returned to normal. Considering the high specificity of positive pathergy test for the diagnosis of Behcet′s disease and the relatively low yield of a leptomeningeal biopsy and DSA in making an alternate diagnosis like primary angitis of the CNS(PACNS),it was decided not to subject the patient for these invasive procedures. Moreover, the steroid responsiveness of the disease being well established, it was decided to go in for a close clinical follow-up after consultation with the family. At two years′ follow-up, patient has remained status quo without any new neurological or systemic symptoms or signs on 20 mg of prednisolone. Discussion We hereby present a patient with steroid responsive acute unilateral subdural effusion and meningoencephlitis with a brainstem lesion that later involved the thalamus. There were no other markers for infective process or systemic vasculitis other than a positive pathergy test. Acute inflammatory subdural effusion has been reported in Kawasaki′s disease, systemic sclerosis and Behηet′s disease. [2],[3],[4],[5] However, in these described cases the subdural effusion was bilateral unlike our patient who had unilateral subdural effusion. Vasculitis of the dural vessels and transient subdural venulitis has been attributed as the possible pathology for subdural effusion in these patients. [3],[5] Varying affection of the dural vessels could account for unilateral effusion seen in our patient. In addition, in our patient the subdural effusion was associated with meningoencephalitis reflected as CSF abnormalities of mixed pleocytosis, marginally elevated protein and normal glucose. The subdural effusion on MRI was hyperintense on T1 and T2WI signifying an exudative nature of the effusion. The subdural effusion could thus be in part a reflection of this meningitic process also. Moderate lymphocytic pleocytosis of CSF has been observed in pathologically proven cases of PACNS and in patients with neurological involvement in Behηet′s disease. [6],[7] The sensitivity of the pathergy test is reportedly low,however, the specificity remains very high for the diagnosis of Behηet′s disease. [8],[9],[10] The sensitivity rates of pathergy test in Indian patients are unknown, but can be assumed to be low.False positivity have been very occasionally reported in non-Hodgkin′s lymphoma, Pyoderma granulosum, CML patients on interferon therapy and hairy cell leukemia,which were all ruled out in our patient. [11],[12],[13] The histopathology from the pathergy site showed neutrophilic infiltration and leucocytoclasia. Leukoclastic vasculitis has been observed in a variety of conditions like autoimmune diseases, infections with streptococci, staphylococci etc,ulcerative colitis,drugs etc which were essentially ruled out in our patient. Biopsy from the pathergy test site has not shown to increase the sensitivity and specificity of the results, 14 but such histopathology is probably more helpful in a very atypical case as ours than a non-standardized pathergy test. The patient did not satisfy the international diagnostic criteria for Behηet′s disease and neurological manifestations as initial presentation of Behηet′s is extremely rare. [15] Gille et al ., reported three patients with initial neurological presentation who developed other classical features months or years later. [16] The MRI in our patient was characterized by brainstem affection that is most consistent with Behηet′s disease. [17],[18] Similar findings may, however, also be expected in other small vessel vasculitis like PACNS. Lymphomatous affection of the CNS also rarely may mimic PACNS. [19] However, on follow-up for two years he remained symptom-free on low-dose steroids, making it unlikely. Conclusion Initial subdural effusion, multifocal neuraxial involvement and meningoencephalitis add to the range of neurological presentation of vasculitis.References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08052f3.jpg] [ni08052f1.jpg] [ni08052f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}