 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
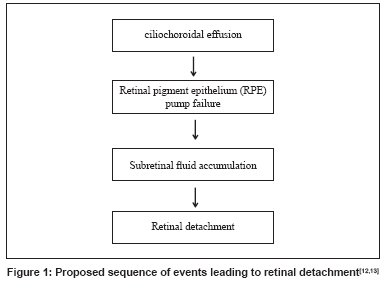
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 204-205 Letter To Editor Retinal detachment presumably associated with topiramate Dey KK, Das S, Mishra A, Guha G The Stroke Unit, Queen Mary's Hospital Sidcup, London Code Number: ni08055 Sir, Topiramate is a sulfamate-substituted monosaccharide. Its usefulness in migraine prevention was shown in several large randomized controlled trials. [3],[4],[5] In this article, we describe two patients who took topiramate as a migraine prophylaxis and subsequently developed retinal detachment. Case 1: This 43-year-old Indian lady was having unilateral frontal and fronto-temporal throbbing headache associated with photophobia and phonophobia since childhood consistent with a diagnosis of common migraine. Her headache was aggravated by travelling, fasting, exposure to sun, sleep deprivation and obnoxious smell. There was no other significant history of any medical or surgical illness. She had mild myopia which was corrected with - 0.5 D glasses. Her migraine was fairly well controlled with 40 mg propranolol, 25 mg topiramate and 10 mg amitryptyline, each once a day. After taking topiramate 25 mg once a day for about a year, she started seeing sudden flashes of lights in both eyes, left being worse than the right in this respect. An ophthalmologic consultation revealed bilateral retinal detachment (RD), left worse than the right in the superolateral quadrant. Her myopia was not any worse and tonometry showed a pressure of 16 mmHg. She underwent barrage laser therapy for the RD. Case 2: This 37-year-old Indian lady suffered from common migraine since her early teens. As she suffered from asthma, beta blocker could not be given as prophylaxis. In fact, she was not on any prophylaxis as the attacks were relatively infrequent. She had myopia which required -1 D corrective glasses. The frequency of her migraine increased as she started taking oral contraceptive pills which she subsequently stopped. She started taking 25 mg of topiramate and her migraine showed dramatic response. On continuation of topiramate 25 mg once a day for one and a half years she started seeing flashes of lights in both eyes. She sought an ophthalmology opinion; lattice degeneration with RD was detected. Her refractive error remained the same but the tonometry showed a pressure of 16 mm Hg on the right and 17 mm on the left eye. She had the encirclage operation. The reported ocular side-effects of topiramate include acute angle closure glaucoma, induced myopia, [6] diplopia and nystagmus, scleritis (including posterior scleritis), oculogyric crisis, blepharospasm, suprachoroidal effusion, myokymia, periocular edema, paraesthesia and periocular pain. [7],[8] Banta et al. , described one case of acute bilateral angle closure glaucoma within two weeks of starting treatment with topiramate. Sankar et al. , reported two cases of angle closure glaucoma: one developed this within two days of topiramate use and the other developed this complication 10 days later. The case described by Rhee et al. , developed bilateral angle closure glaucoma within 24 h of topiramate use. Although Rhee et al. , argued that hypersensitivity reaction to topiramate mediated by prostaglandins caused ciliary body swelling responsible for the glaucoma, Ikeda et al. , pointed out that in all these cases of topiramate-induced galucoma the underlying pathophysiology is one of ciliochoroidal effusion with ciliary body edema. They have coined the term′ ciliochoroidal effusion syndrome′ to portray the series of events leading up to angle closure glaucoma in this context. Anterior rotation of ciliary body and process results from the ciliochoroidal effusion. This in turn leads to anterior displacement of the iris and anterior shift of lens and iris assembly causing the angle closure and narrowing of the anterior chamber. As a result, angle closure glaucoma ensues. Zonular relaxation also leads to thickening of crystalline lens causing myopia. Interestingly, sulfonamides (especially sulphamethoxazole) which share chemical structure with topiramate cause similar ciliochoroidal effusion syndrome. Studies on idiopathic uveal effusion show that longstanding accumulation of choroidal fluid impairs the pump mechanism of the retinal pigment epithelium (RPE) which shifts fluid from inside out. This event leads to subretinal fluid accumulation in the absence of any tears or holes. The subretinal fluid eventually leads to separation of RPE from the neural layer, i.e. retinal detachment (RD). [Figure - 1] illustrates this concept schematically. It is our suggestion that topiramate caused ciliochoroidal effusion in our patients as the initial event. Retinal detachment occurred in our cases 12-18 months after continued use of topiramate during which time ciliochoroidal effusion was likely to decompensate the RPE pump mechanism leading to RD. Notably, in our patients no other explanation for RD, for example retinal breaks and holes (rhegmatogenous RD) or any other source of ciliochoroidal exudates (non-rhegmatogenous RD) was identified by the ophthalmologist and the myopia did not get worse during the course of treatment. It is possible that the lattice degeneration due to myopia also contributed to the process leading up to the RD. We are uncertain as to the mechanism of the retinal detachment in our cases. The myopia was not very severe and it did not get significantly worse while on topiramate, although this may have contributed. We postulate that there is subretinal fluid accumulation by a mechanism similar to that of idiopathic ciliochoroidal effusion syndrome which led to the detachment. While further studies are needed to confirm the pathogenesis we have postulated, it would appear sensible to counsel patients regarding RD and its symptoms before starting topiramate, especially in myopes.[13] References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08055f1.jpg] |
| |||||||||

{kind=link}