 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
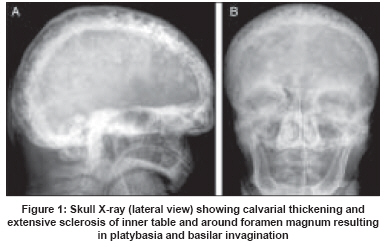
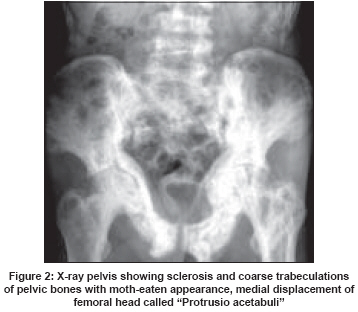
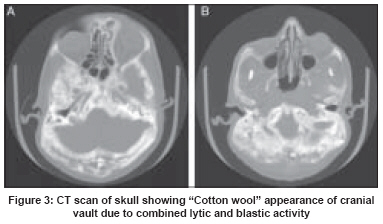
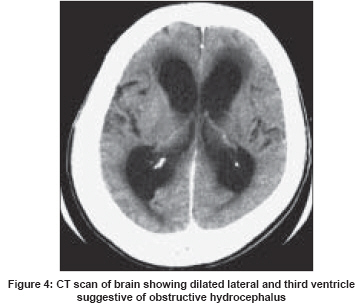
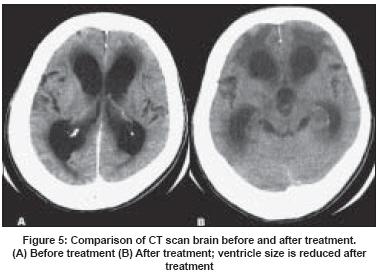
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 216-218 Letter To Editor Paget's disease complicated by hydrocephalus and dementia Pandit Vinay, Seshadri S Department of Medicine, Kasturba Medical College, Manipal Code Number: ni08064 Sir, A 60-year-old male was admitted for evaluation of progressive cognitive dysfunction in the form of memory disturbance, change in personality, mood and behavior, which had gradually worsened impairing his business, social and personal activities for the last four years. Relatives had also noticed difficulty in conversation, poor judgment and decision-making and he needed frequent help. He had urinary incontinence and gait disturbances for few months. He had hearing impairment for the last 10 years. There was no history of any focal neurological deficits, diabetes, hypertension or any significant past medical illness. Examination revealed bounding pulse with wide pulse pressure. Blood pressure was 150/76 mmHg. Neurological examination showed GCS of 9/15, was drowsy and arousable. Mental status questionnaire (MSQ) revealed score of 5/10. Registration, calculation, judgment, recent memory and language functions were impaired. He could understand and perform only few basic commands. Detailed mental status assessment and neuropsychiatric assessment were not possible in view of his sick condition. Motor system examination revealed hypertonia in all four limbs, normal power, exaggerated deep tendon reflexes and flexor plantars bilaterally. Other systems were normal. On investigation, Hb was 14 g%, with blood smear and counts, blood sugars, RFT, LFT, thyroid function tests, Vit B12, folate, Ca, Mg, PO 4 and uric acid being normal. Serology for HIV, HbsAg and HCV were negative. Serum alkaline phosphatase was 2721 IU/l and 24 h. Urine calcium was 209 mg/day. Skull radiograph [Figure - 1] showed marked calvarial thickening and predominant sclerosis of inner table. Sclerosis of the base of the skull was noted around the foramen magnum leading to platybasia and basilar invagination. Spine X-ray showed vertebral sclerosis, coarse trabeculations and pelvic X-ray showed trabeculations with medial displacement of femoral head suggestive of "protrusio acetabuli" [Figure - 2]. Computed tomography (CT) scan [Figure - 3] revealed "cotton wool" appearance of cranial vault due to combined osteoblastic and osteoclastic activity. Dilated lateral and third ventricles with periventricular seepage was noted suggestive of obstructive hydrocephalus [Figure - 4]. Lumbar puncture was normal. Echocardiography showed Grade 1 mitral valve prolapse. BERA showed sensori neural hearing loss. 99 m -Tc bone scan revealed increased uptake in skull, spine and pelvic bones. He was treated with intravenous pamidronate infusion 30 mg/day for three days followed by calcium and Vitamin D supplementation. With treatment, alkaline phosphatase level came down to 1727 IU/l. Patient was also treated with ventriculo-peritoneal shunt and external ventricular drainage. Course of pamidronate was repeated once more. A CT scan was repeated after the above treatments which showed mild reduction in ventricular size [Figure - 5]. Clinical improvement was only marginal and he was discharged at request. Paget′s disease remains asymptomatic in more than 90% of individuals. The most common presentations are bone pain, skeletal deformities, fractures and low back ache. Skull involvement occurs in nearly 40% of cases and the most common presentation is deafness due to compression of eighth cranial nerve and invasion of bony ossicles. [1] Involvement of the base of the skull results in softening of bone with reduced resistance of bone to the weight of the head resulting in flattening and reduction of anteroposterior diameter and basilar invagination. This results in crowding of structures at the posterior cranial fossa leading to various complications. [2] The occurrence of hydrocephalus in Paget′s disease and presenting with the triad of dementia, ataxia and urinary incontinence as that of normal pressure hydrocephalus has been reported by only a few authors so far. [3],[4] Radiologically, basilar invagination is seen in about one-third of patients with skull involvement but development of hydrocephalus is exceedingly rare. The mechanism of hydrocephalus may be due to the obstruction to the flow of the cerebrospinal fluid over cerebral hemispheres or by mechanical displacement of brainstem in relation to the cerebral hemisphere. Paget′s disease is eminently treatable. The new potent bisphosphonates like pamidronate, alendronate, risedronate, not only suppress the disease activity but also can result in prolonged remission. The latest literature recommends zoledronic acid and weekly dosage of alendronate. [5] It is recommended to treat the patients with skull involvement, even if they are asymptomatic, in order to prevent neurological complications. The treatment of choice for patients with hydrocephalus and dementia is ventricular shunting. If shunting is done in the early stage of the disease, good clinical outcome can be expected. [6] Successful outcome, even a dramatic recovery with ventriculo-peritoneal shunt has been described. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08064f5.jpg] [ni08064f2.jpg] [ni08064f1.jpg] [ni08064f4.jpg] [ni08064f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}