 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
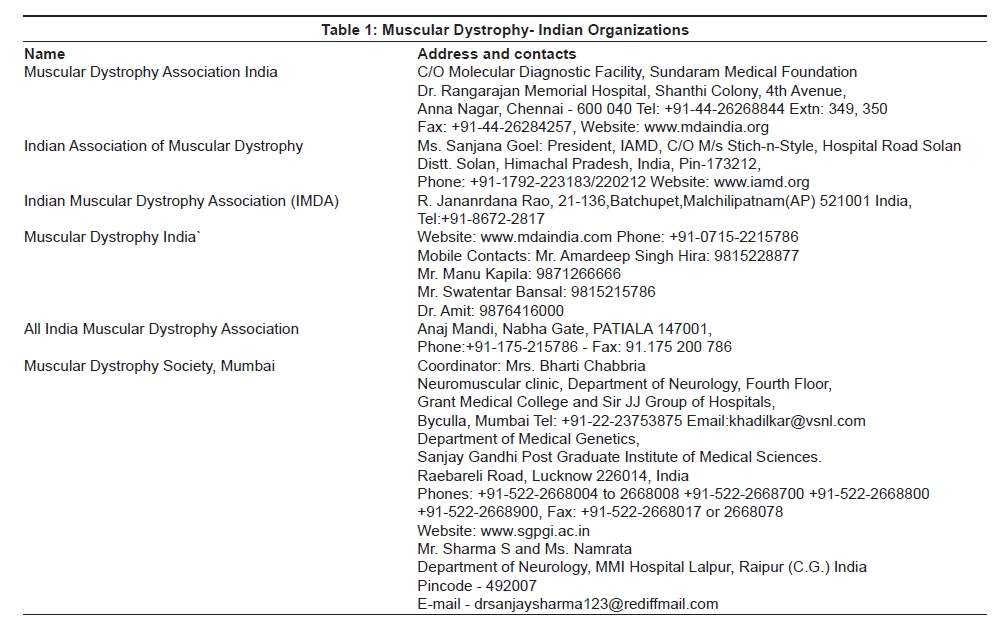
Neurology India, Vol. 56, No. 3, July-September, 2008, pp. 248-253 Review Article Duchenne and Becker muscular dystrophies: An Indian update on genetics and rehabilitation Nadkarni Jayshree J, Dastur Rashna S, Viswanathan V, Gaitonde Pradnya S, Khadilkar Satish V Department of Neuropathology and Applied Biology, Medical Research Centre, Bombay Hospital Trust, Mumbai Date of Acceptance: 15-Sep-2008 Code Number: ni08074 Abstract The application of molecular diagnostic techniques has greatly improved the diagnosis, carrier detection, prenatal testing and genetic counseling for families with Duchenne and Becker muscular dystrophy (D/BMD) in India. The prediction of Duchenne muscular dystrophy (DMD) patients to have out-framed deletions and Becker's muscular dystrophy (BMD) patients to have in-frame deletions of dystrophin gene holds well in the vast majority of cases. Mutation detection is obviously critical for diagnosis but it may also be important for future therapeutic purposes. These factors underscore the need for earlier referral, genetic counseling and provision of support and rehabilitation services which are the main priorities for psychosocial assessment and intervention at medical and social levels.Keywords: Becker′s muscular dystrophy, Duchenne muscular dystrophy, genetics, rehabilitation Introduction Duchenne muscular dystrophy (DMD) is the most common muscular dystrophy in India, like most other parts of the world. Affected individuals suffer long years of increasing disability and their parents go through psychological trauma and face hardships of managing a physically challenged child on day to day basis. The information on the molecular pathology and genetics has been available for over two decades and genetic counseling and prevention can be offered to families at risk. However, issues of illiteracy, social and religious beliefs and the strong Indian desire to have a normal male child pose difficulties in achieving this objective. In the past few years, Polymerase chain reaction (PCR) -based genetic studies have become available in many parts of the country and support groups of parents and medical personnel have begun the efforts to diagnose and rehabilitate the sufferers. This review will discuss the available genetic information and the social and rehabilitative aspects of DMD/ Becker′s muscular dystrophy (BMD) in India.Genetic Aspects of DMD and BMD Both DMD and BMD are caused by a functionally abnormal dystrophin gene which encodes the dystrophin protein. [1] Dystrophin, a rod-shaped 427 kd cytoskeletal protein, regulates the influx of ions into the muscle cell. Absence or inactivation of this protein allows the free inflow of ions into the cell causing severe muscle degeneration. [2] Dystrophin is encoded by dystrophin gene located on the X-chromosome (Xp21.1) and is one of the largest known genes in the human genome (2.5MB gene) having 79 exons and codes for a 14kb mRNA. [1] Probably, due to the large size of the gene, the rate of mutations is high with the majority of mutations being intragenic deletions or duplications. Mutations in this gene result in the most severe lethal form of dystrophy - DMD and its milder variant - BMD. [3] Duchenne Muscular Dystrophy Gene deletions in the Indian Context The deletion analysis of 121 unrelated DMD/BMD patients by PCR analysis as well as Southern blot hybridization from Northern India, [7] observed the frequency of deletion to be 72% although a smaller number of patients was studied. Another group from Northern India which screened 160 cases of DMD from all over India showed 64.4% of patients with intragenic deletions of single exon that did not differ from those with deletion of multiple exons. [8] Most (69.7%) of the deletions involved exons 45-51. Their observations concluded differences no ethnic difference with respect to deletions in the DMD gene. The group from Southern India studied 66 unrelated patients of DMD and observed intragenic deletions in 18 exons and Pm region of the DMD gene using multiplex PCR. [9] Of these, 62.1% showed intragenic deletions. Seventy-eight per cent of the deletions were located at the distal hotspot region (exons 44-55) and 22% of the deletions were located at the proximal region (exons 2-19). Exon 50 was most frequently deleted. They reported that the lower incidence from South India compared to North India, is suggestive of variations in the Southern and Northern population. Molecular basis for reading frame hypothesis The studies on the deletion patterns of BMD and its correlation with reading frame rule and different phenotypes was carried out for 222 patients showing deletions; 88.1% (out-frame) of DMD and 89.1% (in-frame) of BMD conformed to the reading frame rule. [6] However, a North Indian study showed more than 30% deviation from the reading frame rule. [10] The Western Indian study also showed that different phenotypes were sometimes found within families as seen in an index case of a six-year-old boy with DMD phenotype and his maternal uncle with BMD phenotype both with in-frame deletions of exons 45 to 48. [6] Mital et al. , have analyzed the dystrophin gene in 32 unrelated DMD families for the presence of deletions by multiplex PCR for 27 exons and DNA probes for the entire gene. Deletions were identified in 32 patients and the concordance between the clinical phenotype and "reading frame" hypothesis was observed in 24 (75%) cases. [12] Viswanathan et al. (unpublished data) have shown that 60 out of 72 children (83.3%) had DNA deletions involving the central hotspot region of the dystrophin gene (exons 44-45) as carried out by multiplex PCR. Exon 44 followed by 45 was the most common site of deletions. The deletion patterns were studied with reading frame rule and it was observed that 38 out of 49 children (77.5%) showed "out-frame" deletions and 11 (22.44%) showed "in-frame" deletions. The remaining 23 cases had deletions but could not be classified. Thus in this study 76.6% of the patients showed deletions of selected exons as compared to 63.7% shown by Ulgenalp et al. [13] Hence, one of the reasons for deviation from the reading frame hypothesis seems to be at the DNA level which also concurs at the RNA level. Therefore, it is advisable to confirm the mutation on muscle RNA or at the protein level. In a collaborative study, the technique of Multiple Ligation-dependent Probe Amplification (MLPA) has been applied to discern deletions and duplications for all 79 exons. Further, cDNA sequencing was done on MLPA-negative patients to detect mRNA splicing changes. A high rate of large duplications, high rate of exceptions to the reading frame rule and different distribution of mutations in 75 cases of BMD has been reported. [14] Correlation between phenotype and genotype of these DMD patients demonstrates that genetic studies of lymphocyte DNA may not always reflect the situation in the tissue i.e. muscle involved in dystrophin. Whether this is a polymorphism or, related to the disease phenotype needs further confirmation. [14] Carrier detection In DMD In Indian patients, new mutations have been observed including germline mosaicism in 20 out of 29 sporadic mothers, using polymorphic dinucleotide loci for carrier analysis and prenatal diagnosis in deletional DMD families with no previous history of the disease. [16] The carrier detection by DNA-based linkage analysis using highly polymorphic intragenic STR markers was carried out for 327 DMD/BMD patients and out of these, 220 (67.3%) were found to have intragenic deletions and 107 (32.7%) were non-deletion cases. Carrier detection in the female relatives has been carried out in about 25 DMD/BMD families. The authors observed 58-70% informative-ness for central region STRs and 27-47% for 5′/3′ region STRs. They claimed that prenatal diagnosis was successfully provided to five families. [17] Kumari et al. , have analyzed the dystrophin gene in eight DMD and 10 BMD unrelated families (22 subjects) for the presence of deletions by multiplex PCR using 27 exons and Southern hybridization using eight cDNA probes. [18] Deletions were identified in five DMD and seven BMD patients. The concordance between the clinical phenotype and "reading frame hypothesis" was observed in 11/12 patients (92%). Thus the molecular characterization of the dystrophin gene in this study has been useful in advising the patients regarding the mode of inheritance and carrier diagnosis of female relatives, and should also prove useful for prenatal diagnosis. Frequency of Deletions In other Asian Populations The frequency and distribution of deletions of 19 deletion-prone exons clustered in two hotspots in the proximal and central regions of the dystrophin gene were compared in three populations from Singapore, Japan and Vietnam by Lai et al. [19] The most commonly deleted exons at the central deletion hotspot were exon 50 in the Singaporean, exons 49 and 50 in the Japanese and exon 51 in the Vietnamese population. At the proximal deletion hotspot, the most commonly deleted exons were exons 6 and 8 in the Singaporeans, exons 12 and 17 in the Japanese and exons 8 and 12 in the Vietnamese. Similarly, the distribution of dystrophin gene deletions in northeastern China also clusters mainly in two hotspots with neighboring regions of exon 8, which indicates this to be a real hotspot region prone to deletions. [20] The results suggested that although the presence and frequency of the deletions in the two hotspot regions may be similar in the four Asian populations analyzed, the distribution and frequency of deletions among the different exons can vary as a result of population-specific intronic sequences that predispose individuals to preferential deletion breakpoints. Hassan et al. , have studied dystrophin gene deletions in DMD/BMD patients in a Pakistani population and analyzed the frequency and distribution of deletions of 18 exons within the dystrophin gene in 211 unrelated DMD patients. [21] The authors observed that the proportion of intragenic deletions in the Pakistani population is relatively low which is comparable with most of the Asian data. Psychosocial and Rehabilitative Aspects In India the situation faced by DMD patients is afflicted with the unique psychosocial characteristics of Indian society-lack of needed infrastructure to aid these patients in daily living and low level of awareness about the disease amongst medical practitioners and society at large. In the Indian setting, the strong desire to have a normal male child is coupled with religious beliefs and taboos, and poses difficulties for counseling. Many families are willing to look after their DMD sufferers but continue to procreate with the fervent wish for a normal son. Thus, authors have seen up to six DMD siblings in one family. Alternative medical systems like Ayurveda, Unani medicine, Homeopathy and other folk medicines are resorted to along with allopathy and it is very common for patients to turn to one or more of them when allopathy does not offer a cure. Study of the psychosocial aspects of DMD Patients exhibited poor self-image and mild to moderate depression. Immobility led to social alienation and profound isolation. In turn this led to increase in perceived parental stress and diminished the effectiveness of parental support and encouragement. This put them at greater risk of psychological maladjustment and this second handicap posed a significant mental health problem. Impact of the second handicap has been elucidated previously in the Western literature. [23],[24] Interpersonal relationships in these families were peculiar in that there was strong identification forming a close-knit unit, which nonetheless suffered social isolation. However, such preoccupation with the family, with its pervasive sharing of feelings of helplessness and guilt suppressed open communication about the disease implications. [22] All these factors underscore the need for psychosocial assessment and intervention at medical and social levels. [24] In the rehabilitation of patients with DMD, proper assessment of disabilities is essential. This requires specialized approach. In a study form Bangalore, 31 patients with DMD of age four years and above were studied. The motor functions were evaluated using total motor score, upper and lower extremity function grades and timed function tests. Disability was quantitated with Barthel index. Children were found to have disabilities in multiple spheres of life, which were significantly influenced by the motor power. Barthel index was useful in identifying and quantifying specific areas of disabilities in these children. [25] Support groups have formed to help the rehabilitation of DMD and BMD patients in India. The groups undertake camps for the affected individuals and their caregivers provide physiotherapy and orthotics services and liaise with the medical specialists for advice. A list of Indian organizations working for muscular dystrophy, appearing on the internet, has been presented in Table 1. Rehabilitation program for Duchenne muscular dystrophy at Mumbai Management of Duchenne Muscular Dystrophy at Chennai On the clinical side MDA India is fortunate to be part of the Cooperative International Neuromuscular Research Group (CINRG) over the last five years and has been participating in some multi-center clinical trials. This collaboration has helped us in setting up a molecular diagnostics facility at Chennai for the diagnosis of DMD as well as carrier analysis. All this had led to the formation of a vibrant team involving physiotherapists, dietician, psychologist, molecular biologists, clinical research coordinator, social workers and volunteers apart from the pediatric neurologist. Most of the personnel involved have had training and exposure to what happens in some of the best centers of excellence in the world as regards each of their disciplines. This team is therefore able to share their knowledge and skills with the families of children with DMD in their area of expertise. Hence, these studies on molecular diagnostic approaches and the usefulness of the rehabilitation programs will be very beneficial to analyze the needs of patients with DMD/BMD and to develop strategies to improve the management of the disease. Conclusion DMD and BMD, common and important muscular dystrophies in India, have been characterized genetically in various centers in India. The results of the genetic information are largely similar across the country with some regional variations and follow the pattern seen in other Asian countries. The information on reading frame hypothesis is being explored with local and collaborative efforts and carrier detection has become available in select centers. Support groups are vital in the management of this disease and its chronic disability. Regional groups are currently working for this objective. Illiteracy, cultural and social issues in India pose unique challenges in these disorders. There is a need for further comprehensive efforts for the accurate molecular diagnosis, carrier detection, prenatal diagnosis, genetic counseling and rehabilitative measures on a large scale in India.References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08074t1.jpg] |
| |||||||||


{kind=link}