 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
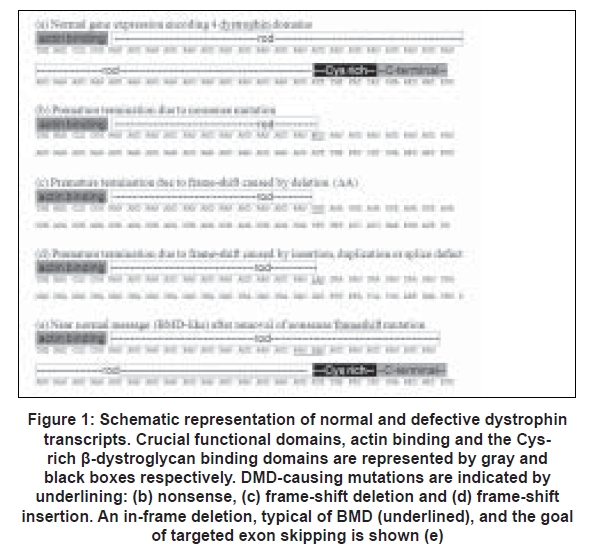
Neurology India, Vol. 56, No. 3, July-September, 2008, pp. 254-262 Review Article Exon skipping and Duchenne muscular dystrophy: Hope, hype and how feasible? Wilton Steve D, Fletcher Susan Centre for Neuromuscular and Neurological Disorders, Molecular Genetic Therapy Group, University of Western Australia Date of Acceptance: 24-Jul-2008 Code Number: ni08075 Abstract Duchenne muscular dystrophy (DMD), the most common and serious form of childhood muscle wasting is generally caused by protein-truncating mutations in the large DMD gene. Specific removal of an exon from a defective DMD gene transcript has the potential to allow synthesis of a semi-functional dystrophin, thereby reducing the severity and presumably progression of muscle wasting. The efficacy of this treatment will vary greatly between the different mutations that preclude the synthesis of a functional dystrophin. Restoration of the reading frame from a large multi-exon genomic deletion, typically greater than 36 exons, may lead to synthesis of a protein with only partial function and limited clinical benefit, whereas excising a nonsense mutation in a redundant exon should generate a near normal dystrophin. A clinical trial has recently confirmed proof-of-principle that exclusion of Exon 51 from human dystrophin mRNAs, carrying frame-shifting deletions adjacent to this exon, results in dystrophin expression. No major side-effects after local administration of the antisense oligomer were reported. Additional trials are underway, targeting the same exon but using an oligomer of different backbone chemistry. If functional dystrophin synthesis is demonstrated, and safety issues are addressed, subsequent trials will involve systemic delivery. Great challenges are ahead, some technical; establishing an effective delivery regimen, some ethical; choosing subsequent targets for therapy, and others of an administrative and regulatory nature.Keywords: Becker muscular dystrophy, clinical trials, Duchenne muscular dystrophy, exon skipping, morpholino oligomer, personalized genetic medicines Background Duchenne and Becker muscular dystrophy (DMD and BMD) are allelic muscle wasting conditions arising from mutations in the large DMD gene at Xp21.2. [1] The most common, serious and progressive form, DMD, is caused by inactivation of the DMD gene product. Affected individuals appear normal at birth and clinical symptoms may be observed between the ages of two to three years. Approximately 50% of DMD males do not walk until after the age of 18 months, and exhibit signs of retarded motor development, including a waddling gait, difficulty running and jumping and calf enlargement. Muscle wasting is relentlessly progressive in a symmetrical fashion, with joint contractures an important clinical sign. As the process of muscle regeneration becomes overwhelmed, regenerating fibers are less frequent and the replacement with adipose and connective tissue contributes to pseudo-hypertrophy of some muscles. Affected individuals are typically non-ambulant by the age of 12 years, and in some cases as early as seven years (review, [2],[3],[4] ). Contractures develop as the disease progresses, and in the absence of optimal care, including corticosteroid treatment, physical therapy and nocturnal assisted ventilation, [5] most patients succumb to the disease by the age of 20 years as the result of respiratory and/or cardiac complications. In contrast, BMD patients present with a spectrum of severity, from borderline DMD to asymptomatic. [6],[7] It has been estimated that BMD occurs at only 10% the incidence of DMD, most likely through the inability to recognize and diagnose particularly mild cases prior. [4] Although many BMD individuals present with some symptoms between the ages of five to 15 years, by definition a BMD patient will remain ambulant until age 16 years or longer. Some patients despite a deletion within the dystrophin coding sequence, present with no evidence of pathology, or elevated serum creatine kinase, a sensitive marker of muscle damage. [8] The reading frame rule, proposed by Monaco et al. , tends to hold true for the majority of DMD and BMD cases. [9],[10] Duchenne muscular dystrophy-causing mutations, either frame-shifting deletions or duplications, nonsense mutations or splice motif errors lead to the loss of a functional DMD gene product. Becker muscular dystrophy typically results from in-frame deletions in the DMD gene that allow synthesis of an internally truncated, but functional protein. [9],[10] The variation in severity reflects the extent and location of the deletion. Large multi-exon deletions or the loss of crucial functional domains typically lead to the more severe phenotype, whereas loss of in-frame exons within the central rod domain appears to have little or no consequences. [11],[12],[13],[14],[15] The general rule is that the loss of 36 or more exons is associated with a severe phenotype, regardless of the reading frame, suggesting a minimum size for functional dystrophin. [16] The lack of dystrophin disrupts the link between the actin cytoskeleton and basal lamina, compromising the sarcolemma (review, [17] ). Dystrophic muscle fibers are prone to injury during force generation and repeated damage leads to muscle loss and subsequent fibrosis. However, rare dystrophin-positive fibers accumulate in muscles of many DMD patients and in animal models of muscular dystrophy. [18],[19],[20] This remarkable phenomenon is the result of naturally occurring alternative dystrophin transcripts that bypass the DMD gene lesion. Although the precise mechanism is unknown, the loss of multiple exons from the mRNA, flanking the DMD genomic deletion, has the potential to restore the reading frame of the dystrophin transcript in the revertant fibers. [21],[22],[23] In the mdx mouse, an animal model of muscular dystrophy, this mechanism generated in-frame DMD gene transcripts missing multiple exons, typically 20 or more, including Exon 23 that contains the dystrophin inactivating nonsense mutation. [24] The skeletal muscle-specific dystrophin isoform plays a crucial role, stabilizing the sarcolemma [17] through the functional domains, the primary actin-binding sites at the amino terminal encoded by Exons 2, 4 and 5, and weak actin binding between exons 35 and 44, and the cysteine rich b-dystroglycan binding site encoded by Exons 62-69. [25] The central rod domain appears to be variably dispensable, as demonstrated by the mutations in mildly affected or asymptomatic BMD patients, [6] and the existence of naturally occurring revertant fibers. Hence, a logical strategy to reduce the severity of DMD caused by dystrophin-truncating mutations is to manipulate primary gene transcript processing so as to produce an in-frame mRNA capable of being translated into a functional BMD-like protein. [22] Dystrophin: An Ideal Candidate for Transcript Manipulation Manipulation of dystrophin pre-mRNA processing might appear a formidable challenge, considering the size and complexity of expression of this gene. The strategy demands that one or two exons be excluded from a 2.4Mb DMD gene transcript during the simultaneous expression and processing of thousands of other gene transcripts. However, many DMD gene features that have proved a challenge to cell and gene replacement or repair therapies for DMD are regarded as positive attributes for transcript manipulation, termed ′exon skipping′. The DMD gene is the largest known and consists of 79 exons spanning some 2.4 Mbp, [26] much too large to be incorporated into viral vectors currently available for clinical applications. The wild type protein-coding region is in excess of 11 Kb, incompatible with the capacity of most viral vectors. The identification of a very mildly affected BMD patient with an in-frame deletion of almost half the gene prompted the construction of a vector containing the dystrophin "minigene". [27] Elegant studies have shown that multiple dystrophin domains can be trimmed to create microdystrophin isoforms. [28],[29],[30] These constructs are compatible with current viral vectors, lending impetus to gene replacement studies and confirming that there are conditionally redundant domains within the dystrophin protein. [31] Detailed studies have shown that restoration of micro-dystrophin expression at the sarcolemma does not necessarily correlate with functional rescue. [32] Under the control of multiple promoters, the predominant dystrophin transcript is expressed in skeletal muscle as a mature 14 kb mRNA. [1],[25],[33] It has been estimated that 16 h elapse during the processing of a single dystrophin pre-mRNA, during which time 79 exons must be spliced from the primary gene transcript. [34] Possibly because of this major effort in gene processing, the mature DMD gene transcript is present at very low levels and has been estimated to only constitute 0.01-0.001% of the total mRNA. [35] The full length transcript encodes a protein with four major domains and the reading frame is represented in cartoon form in [Figure 1a]. The most common type of dystrophin mutation is a deletion of one or more exons, which may disrupt the reading frame with catastrophic consequences. [10],[36] However, nonsense mutations where a single base change alters a codon into a premature protein-termination signal [Figure 1b], micro-insertions/deletions to disrupt the reading frame [Figure 1c] or nucleotide changes that disrupt pre-mRNA processing so that an exon is lost, or intronic sequences are retained in the mature mRNA [Figure 1d] have been reported. A BMD-like gene message is depicted in [Figure 1e], where the removal of the "END" nonsense mutation, or the "ND" frame-shift bypasses the gene lesion, and permits the rest of the gene message to be translated. Targeted Exon Skipping Some 15 years ago, Kole and colleagues directed antisense oligomers (AOs) with 2′-O-methyl modified bases on a phosphorothioate backbone (2OMeAOs) to cryptic splice sites that arose from intronic mutations in the b-globin gene. [37] Upon masking the cryptic splice site, the splicing machinery defaulted to recognition of the normal b-globin splice sites. Induced dystrophin exon skipping is similar in principle, except that normal splice motifs are targeted to mask the exon from the splicing machinery, leading to exclusion of the exon from the mRNA. In this manner, a nonsense mutation can be removed or the reading frame can be restored around deletions or insertions in the DMD gene transcript. Although exon skipping is the most common consequence of splice motif mutations, some splice defects lead to the activation of one or more cryptic splice sites. In the golden retriever model of muscular dystrophy (GRMD), [38] the majority of dystrophin transcripts are out-of-frame, since the intron 6 acceptor splice site mutation results in loss of Exon 7 from the mature mRNA. [39] However, sensitive and specific PCR conditions detected near normal length dystrophin transcripts containing all but the first five bases of Exon 7 as some transcripts arose from the recognition of the first AG in Exon 7. [40] Had this transcript been in-frame, it is possible that the severity of the disease may have been mitigated somewhat in these dogs. Human dystrophin splice site mutations and activation of cryptic splice sites have been reported, including one in intron 26 which appears to have arisen independently at least twice (www.dmd.nl). [41] Early studies We commenced dystrophin exon skipping studies using the mdx mouse, [52] an animal model carrying a nonsense mutation in dystrophin Exon 23. [53] Although the mdx mouse is commonly referred to as a model of DMD, this is not strictly accurate, since these animals do not present the severe muscle wasting seen in DMD boys. Despite this limitation, the mdx mouse offers an excellent molecular model of a dystrophin mutation, and through detailed histological studies, it is apparent that the diaphragm develops severe dystrophic pathology as the animal ages. [54] We transfected three 2OMeAO cationic lipoplexes into primary mdx myogenic cells. [55] The scrambled AOs and the oligomer directed at the acceptor splice site had no detectable effect on dystrophin pre-mRNA processing. However, the 20mer directed to the donor site was able to induce Exon 23 skipping in a dose-dependent manner. A series of overlapping AOs were subsequently designed to both donor and acceptor sites and, while the acceptor remained an unresponsive target, the efficiency of exon skipping was improved by selecting a 20mer targeted to the donor site. [56],[57] The use of a block, co-polymer F127 resulted in functional amounts of dystrophin expression in the tibialis anterior after intramuscular delivery of the same AO. [58] Other formulations have also been shown to enhance 2OMeAO delivery. [59],[60],[61],[62] DNA oligomers are of limited potential for induced exon skipping, since this chemistry induces RNase H activity, leading to mRNA degradation. Perhaps more significantly, oligomers of this chemistry will be rapidly degraded by nucleases. [63] Although 2OMe AOs have proved most effective, since they are more nuclease resistant and do not support RNaseH activity, several other oligomer chemistries have been evaluated, including peptide nucleic acids (PNAs), [64],[65],[66] locked nucleic acids (LNAs), [64],[67] 2′-O-(2-Methoxy)ethyl-modified (MOE) [65] and phosphorodiamidate morpholino oligomers (PMOs). [68],[69] The PNAs were not initially reported to be effective, [64],[68] however, a recent report showed some exon skipping. [66] The LNAs induced robust exon skipping, but the exceedingly high Tm indicated great potential for off-target effects due to cross-annealing to related sequences, [64] This group reported that PMOs were not effective and that 2OMeAOs were the preferred chemistry for clinical application. Oligomer Delivery Although in vitro uptake of 2OMeAO cationic lipoplexes into myogenic cells is efficient, these compounds have poor uptake in the absence of delivery reagents. To facilitate a comparison between 2OMeAOs and PMOs, we annealed a sense strand leash to the PMO, thereby allowing the duplex to be complexed with a cationic liposome, before transfection into cultured cells. [69] It became apparent that while uncomplexed PMOs were not taken up efficiently in vitro , PMO:leash:cationic lipoplexes induced robust and sustained exon skipping. The PMO uptake by cultured cells after application at high concentrations and scrape loading to facilitate uptake has been reported. [70] We reported that a single intramuscular injection of a PMO in saline was able to induce strong dystrophin expression, six weeks after administration. [68] The compound, injected into 11-day-old mice before the peak of muscle degeneration at 18-21 days, [71] was able to prevent muscle breakdown, as evidenced by normal muscle morphology and a statistically significant reduction in fibers with central nucleation, a marker of muscle regeneration. Subsequent reports showed that systemic delivery of the PMO into the mdx mouse restored dystrophin expression in skeletal and smooth muscle, although the heart was refractory to treatment. [68],[72] A major improvement in the efficacy of exon skipping after systemic delivery was achieved through the use of PMOs coupled to cell-penetrating peptides. [73],[74] The ability of PMO-peptide conjugates to induce exon skipping has been demonstrated in vitro , including human and mouse muscle explants, [75] GRMD canine model of muscular dystrophy [76] and the mdx 4 CV[77] mouse model (Mitrpant, unpublished data). Body-wide dystrophin expression was restored in mdx mice by intraperitoneal administration of the PMO-cell-penetrating peptide P007 conjugate as four, once-weekly doses of 5 mg/kg. [73] Although exon skipping was not demonstrated in cardiac muscle, the reduction in skeletal muscle damage lowered the serum creatine kinase to near-normal levels. Recent development of a peptide that mediates PMO-induced exon skipping in cardiac muscle has removed the remaining barrier to effective systemic dystrophin restoration. [78] Numerous peptides were screened in an elegant transgenic mouse model and the most promising candidate was then evaluated for delivery of the PMO targeted to dystrophin Exon 23 in the mdx mouse. There is no evidence of immune responses to the peptides to date (unpublished data), but further investigation into nonspecific or toxic effects is ongoing. Target Site Selection and Oligomer Design Although in vitro studies evaluating human dystrophin exon skipping and work in animal models have proved promising, there are four major challenges to exon skipping therapy for DMD that must be overcome. Achieving effective system delivery has been an obstacle to many nucleic acid therapies, as is selection of an oligomer chemistry that can safely induce sustained re-direction of dystrophin expression after long-term administration. In addition, it will be necessary to design many different oligomers to restore the reading frame around mutations, including non-deletion mutations, across the DMD gene, and undertake safety and toxicology studies. The oligomers designed to excise selected dystrophin exons in three animal models of muscular dystrophy, mdx and mdx 4 CV mice and the GRMD dog, have not provided us with any obvious parameters for optimal targeting. A donor splice site was most amenable when targeting Exon 23 for removal from the mdx mouse DMD gene transcript, while canine dystrophin Exons 6 and 8 were excised by oligomers directed to ESEs and the acceptor site respectively. Mouse dystrophin Exons 52 and 53 could only be efficiently removed using a combination of two and three AOs respectively (unpublished data). Every dystrophin exon, excluding the first and last, can be excised from the mature human DMD gene transcript. Aartsma Rus and colleagues [47] reported on 114 oligomers that were evaluated for the excision of 35 dystrophin exons. We reported a preliminary draft of AO sequences capable of removing each human dystrophin exon and found that a substantial proportion of compounds could induce some exon skipping, albeit to a variable degree. [79] Some AOs could induce readily detectable exon skipping after in vitro transfection as lipoplexes at concentrations of 10 nM, while others induced sporadic or very low levels of exon skipping after administration at 600 nM. Clearly, the most applicable compounds for the clinic will be those that are effective at the lowest concentrations, with more easily achievable therapeutic thresholds and lower risk of off-target effects. We, and others have shown that an oligomer may induce targeted exon skipping, even when the compound includes mismatches. [64],[80] We demonstrated skipping of Exon 19 from the human and mouse dystrophin transcripts using mismatched AOs, but only at high concentrations. Clearly, cross-reaction to related sequences is a possibility and it will be most important to design effective compounds that excise the target exon at low concentrations. We reported that displacing an oligomer by a few nucleotides dramatically alters exon skipping activity. [80],[81] Consequently, we have devoted considerable effort to design oligomers capable of inducing robust exon skipping at low concentrations, and it has become apparent that targeting obvious splice motifs will not guarantee induced exon skipping. [79] Despite early success in excluding Exon 23 from the mouse dystrophin mRNA by targeting the donor splice site, [55],[56],[57] directing an oligomer to the identical coordinates in the human DMD gene transcript had no effect on dystrophin processing. [81] Indeed, the human donor splice sites are not generally preferred targets, with only two exons out of the 77 having donor splice sites as the optimal target motif [79] and the majority of exons were efficiently removed by oligomers directed to ESEs, intra exonic motifs that enhance exon recognition. A small number of exons that proved difficult to remove showed satisfactory levels of exon skipping when targeted by combinations of oligomers. [82],[83] The effect of AO cocktails is clearly synergistic, as particular AOs that are ineffective individually can induce exon skipping when applied at very low concentrations. [83] The AO length emerged as playing an important role in oligo design. In many cases, increasing the length from 25 to 30 nucleotides conferred substantial increases in exon skipping efficiency, far outweighing the additional cost synthesis. [81] Increasing one oligomer from 25 to 30 nucleotides increased exon skipping efficiency fourfold, [81] however, oligomer length must be determined on an exon-by-exon basis. Increasing the length of the oligomer targeting the mouse dystrophin Exon 23 donor site from 25 to 30 bases was counterproductive. Our data suggests that the optimal oligomer length for exon skipping is between 23 and 30 nucleotides, regardless of whether the 2OMeAO or PMO chemistry is used. [81],[83] Exon Skipping: Clinical Implementation In the first reported clinical trial of exon skipping for DMD, a DNA oligomer targeted to Exon 19 was administered intravenously to a single DMD patient missing dystrophin Exon 20. [84] Despite showing appropriate dystrophin exon skipping in lymphocytes, induced Exon 19 skipping and restoration of dystrophin synthesis in muscle appeared equivocal. Several parameters could have contributed to this, including the nature of the oligomer chemistry, dosage, timing and duration of the regimen. More recently, a Phase Ia trial not only addressed the primary safety concerns but also conclusively demonstrated restoration of dystrophin expression in the most common subset of DMD deletion mutation patients. [85] Intramuscular injection of a 2OMeAO (PRO051) targeted to Exon 51 was carried out in four DMD individuals with different deletions in the major mutation hotspot. Excision of Exon 51 restored the reading frame in all participants, and dystrophin expression was unequivocally demonstrated at the site of injection by immunofluorescence, Western blotting and RNA studies. A Phase I trial of a PMO targeting Exon 51 [86] is ongoing, and as yet, no data is available. This protocol differs from that by van Deutekom et al. , [85] in terms of chemistry, oligomer sequence and target muscle. Non-deletion Mutations Exon skipping development has focused on restoring the reading frame for the most common type of dystrophin mutation: genomic deletions. Exon 51 was selected as the target for the first clinical trial, because removal of this exon would benefit a large percentage of DMD patients. However, exon skipping can be applied to other types of dystrophin mutations, and perhaps it would be more accurate to consider exon skipping as a generic platform of intervention for DMD. Although genomic deletions of one or more exons are the most common DMD-causing mutations, cases arising from exonic duplications, nonsense mutations, splice motif detects, micro-insertions or deletions may be more amenable to exon skipping. Aartsma-Rus and colleagues [87] recently restored the reading frame in DMD patients with genomic duplications. If one copy of a single-exon duplication could be removed, the resultant dystrophin transcript should be translated into a normal protein. Although apparently simplistic, this may prove a technical challenge. It would appear that targeting a duplicated exon generally results in the removal of both exons from the transcript, leading to disruption of the reading frame unless additional exons are removed (Wilton, unpublished observations). [87] Generation of normal transcripts from other DMD dystrophin genes by selected exon exclusion is possible. Pseudo-exon incorporation in the mature DMD gene transcript arises from intronic base changes which activate a set of cryptic splice motifs that meet the criteria for exon recognition. The excessive intronic component of the DMD gene may contribute to the incidence of pseudo-exons as a cause of DMD, reported to occur at a frequency of up to 4%. [88] Despite the rarity of pseudo-exon inclusion, such mutations are perhaps ideal candidates for exon skipping, since exclusion would result in a normal dystrophin mRNA. [88] We reported a novel dystrophin re-arrangement involving an un-equal inversion of 28 kb spanning Exons 49 and 50 that led to the loss of two exons from the mature gene transcript and the variable inclusion of several pseudo-exons from the non-coding strand. [89] Of the two predominantly incorporated pseudo-exons, one was very efficiently excluded by several oligomers targeting various motifs predicted to be involved in exon recognition and incorporation. In contrast, the other commonly incorporated pseudo-exon could not be dislodged from the dystrophin mRNA with any of the oligomers designed to target that exon. However, this recalcitrant pseudo-exon was efficiently removed with an oligomer targeted to the adjacent Exon 51. Clearly, each exon and dystrophin mutation will need to be addressed on a case-by-case basis. While suppression of pseudo-exon inclusion should result in a highly functional dystrophin, protein-truncating defects in the large central rod domain of dystrophin, such as nonsense mutations, micro-insertions or deletions, should also result in near-normal dystrophins. Addressing such mutations in much of the rod domain would only require removal of the defective exon, as exclusion of any exons from 23 to 42 will not disrupt the reading frame, and the loss of an exon in the rod domain would be expected to generate a dystrophin of near-normal function. Few BMD patients have been identified with deletions in this region, implying that such mutations either do not occur, which is unlikely, or manifest as near-normal phenotypes and are not commonly diagnosed. If exon skipping is considered as a personalized genetic therapy, the frequency of each DMD mutation must not be a parameter in determining which exons should be considered as priority targets. Restoration of the reading frame in some cases of DMD, with a primary gene lesion of the loss of 36 or more exons, may allow eventual synthesis of a dystrophin with normal amino and carboxy termini, but the massive internal deletion results in a heavily compromised dystrophin. Alternative Exon Skipping Therapies One perceived limitation of oligomer-induced exon skipping is the need to periodically re-administer the compound to maintain therapeutic levels of dystrophin. The frequency of re-administration will depend upon many factors; the efficiency of target exon removal, the stability of the oligomer chemistry that determines biological persistence of exon skipping and the functionality of the induced dystrophin in stabilizing the sarcolemma and muscle fiber. Several approaches to sustained exon skipping without the need for periodic administration of chemically synthesized oligomers are under consideration. Targeted gene modification using a variety of correcting molecules, including chimeric oligomers, [90],[91] single-stranded DNA oligomers [92] or PCR fragments through short fragment homologous recombination [93] has been reported. Since exon skipping is generally the most common consequence of splice motif mutations, appropriate and effective induction of mutations in donor or acceptor splice sites could bypass many DMD mutations. Targeted disruption of the intron 22 acceptor splice site, with the aim of excluding Exon 23 has been achieved. [92] However, instead of generating precise Exon 23 skipping, multiple transcripts excluding several exons were detected. Oligonucleotide mutagenesis is still under development and is limited by very low rates of DNA modification, particularly in vivo. Exon skipping has been induced by viral expression cassettes, which promote transcription of antisense sequences. [94],[95],[96] Long-term dystrophin expression was demonstrated after systemic delivery of the recombinant adeno-associated virus in the mdx mouse [95] and in canine muscle [97] and while exceedingly promising, this approach will face the same challenges as conventional gene replacement therapies, including scale-up of production, immune response to the vector and regulatory approval. Ex vivo genetic transformation of mouse and patient cells with viral expression cassettes tailored to correct the reading frame of the dystrophic line, followed by transplantation, has been reported. [98] The fusion of cell, gene and genetic therapies, while elegant and highly innovative, faces substantial additional challenges resulting from the combined limitations of each strategy. Summary We anticipate that several different clinical trials evaluating induced exon skipping mediated by synthetic oligomers will commence over the next few years, if the current challenges can be adequately addressed. Should oligomer-induced exon skipping be regarded as a platform technology, and the oligomers are considered class-specific compounds, there is the potential to quickly address many different amenable mutations. However, there are few relevant animal models, and the introduction of an oligomer to excise an exon, e.g. dystrophin Exon 51, may induce dystrophic pathology in a normal animal. Similarly, dystrophin Exon 51 skipping cannot be studied in normal human volunteers, since the loss of this exon would lead to DMD. There is general agreement that systemic oligomer delivery is mandatory, however, the most effective compound reported to date, the PMOs coupled to cell-penetrating peptides is yet to be validated in humans. Personalized genetic medicine is an emerging concept, and as such, would be expected to face challenges. The only pharmacological therapy shown to be of benefit to DMD patients, corticosteroid treatment, is beset by significant side-effects and the debate continues as to the best administration regimen, even though the commonly used steroids have been clinically available for three decades. We hope that it does not take a similar period of time to establish exon skipping modalities and demonstrate that the AOs can reduce the severity and progression of DMD. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08075f1.jpg] |
| |||||||||

{kind=link}