 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
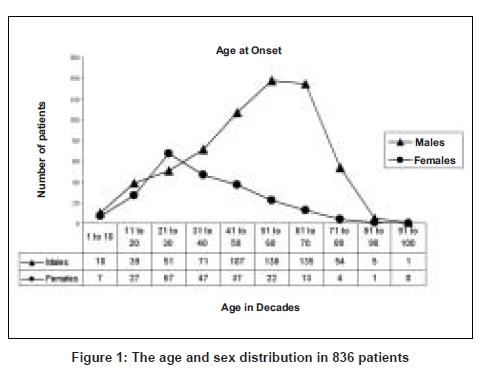
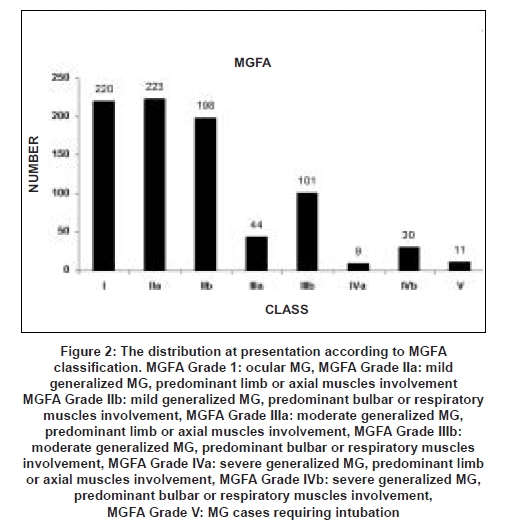
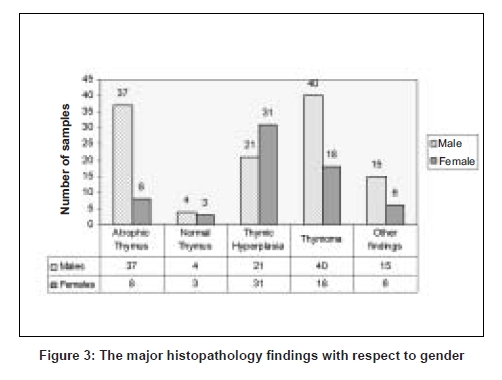
Neurology India, Vol. 56, No. 3, July-September, 2008, pp. 352-355 Original Article Myasthenia gravis: A study from India Singhal BS, Bhatia Nisha S, Umesh T, Menon Suresh Department of Neurology, Bombay Hospital Institute of Medical Sciences, Mumbai - 400 020 Date of Acceptance: 22-Sep-2008 Code Number: ni08087 Abstract Background: We present the findings from the largest hospital-based studies on myasthenia gravis from India, using data collected over a period of 43 years from the Neurology Department in a tertiary referral center in India.Objectives: To study the clinical presentation, age at onset, gender distribution, serological status and thymic pathology in patients with myasthenia gravis. Materials and Methods: A retrospective study was carried out using records of patients with myasthenia gravis from the years 1965 to 2008. Results: Of 841 patients, 836 (611 males and 225 females) had acquired myasthenia (myasthenia gravis) and five congenital myasthenia. The median age at onset was 48 years (males 53 years and females 34 years). The peak age at onset for males was in the sixth and seventh decade and in females, in the third decade. Two hundred and twenty-two (26.31%) patients had ocular and 616 (73.68%) generalized myasthenia. Serological studies were done in 281 patients with myasthenia gravis for Acetylcholine receptor (AchR) antibodies of which 238 (84.70%) were seropositive. The most common histopathology was thymoma and the second most common was thymic hyperplasia. Conclusion: Myasthenia gravis in our study was more common in males (M:F of 2.70:1). There was a single peak of age at onset (males sixth to seventh decade; females third decade). The higher prevalence of thymomas in this series is in all probability related to selection bias as patients with thymic enlargement or more severe disease underwent thymectomy. Thymoma was more common in males; hyperplasia in females. Keywords: Acetylcholine receptor antibodies, congenital myasthenia, myasthenia gravis, thymoma Introduction Myasthenia gravis is a potentially serious but treatable autoimmune disease affecting the neuromuscular junction of the skeletal muscle. It is characterized by weakness and fatigability of the voluntary muscles and is, in most patients, caused by auto antibodies against the muscle nicotinic acetylcholine receptors (AchR). [1] There is a lack of epidemiological data from India. We present findings from our data (collected over 43 years from 1965-2008) from a single tertiary referral center in India.Materials and Methods All the patients included in the study were cases of myasthenia diagnosed on clinical basis and response to cholinesterase inhibitors (edrophonium or neostigmine). Chest X-ray was done in all patients. Electrophysiology, serology, Computed Tomography (CT)/Magnetic Resonance Imaging (MRI) of chest were done when these became available. The data was analyzed retrospectively with respect to gender, age at onset, Myasthenia Gravis Foundation of America (MGFA) classification and results of investigations including serology, electrophysiology, and histopathology of thymectomy specimens. All the patients included in the study were evaluated and treated by one of the authors over a period of 43 years. Electrophysiological studies The distal compound muscle action potential was recorded and when found to be ambiguous; a 10 sec post exercise response was recorded to rule out any increment due to a presynaptic neuromuscular transmission defect. Concentric needle electromyography examination was done in some patients to rule out any primary muscle disease or anterior horn cell lesion. Single fiber electromyographic studies were not done. Antibody assays Thymectomy Depending on the size of the thymus, transcervical or transternal thymectomy was done. Indications for thymectomy were thymic enlargement or tumor documented on radiology. In non-thymomatous patients, the indications were severe and progressive generalized disease with suboptimal response to anticholinesterase drugs and no major contraindications to surgery. Results Age at onset and sex distribution In the acquired group, the peak age at onset for males was in the sixth and seventh decade with 138 (22.58%) in the sixth decade and 135 (22.09%) patients in the seventh decade. In females, the disease presented early with a peak age at onset in the third decade with 67 (29.77%) patients [Figure 1]. MGFA classification Immunological findings Electrophysiology Thymectomy and thymic histology Discussion There are several studies from India dealing with various aspects such as electrophysiology, [3] response to various treatment modalities [4] and comparison of juvenile with adult myasthenia. [5] However, there is no epidemiological data on myasthenia from India. The present study, although not an epidemiological study, is the largest study from a tertiary referral center in India. Myasthenia gravis has traditionally been regarded as a disorder of young women and older men, with the disease being more prevalent in females. Studies from Greece, by Poulas et al., and Cambridgeshire by Robertson et al., showed a F:M ratio of 1.41:1 [6] and 2:1 [7] respectively. In Asia, epidemiological studies on Hong Kong Chinese by Yu et al. , showed a F:M ratio of 2.1:1. [8] There was a female preponderance in all these studies. In contrast, we found a male preponderance; the M:F ratio being 2.70:1. Interestingly, Wing Lok et al. , in their hospital-based study from Singapore noted myasthenia to be four times more common in Indian males than females although in their ethnic Chinese and Malay patients there was a female preponderance. [9] The male preponderance in our study cannot be explained by the population statistics of India alone, which showed a F:M ratio of 1:1.01. [10] As socio-culturally, men have easier access to tertiary healthcare than women in India, it is possible that mild cases of myasthenia gravis in females may have gone unreported. Myasthenia gravis affects all ages but not uniformly. In several studies there is a bimodal distribution of age at onset for females and males. In the female population, Wing Lok et al., from Singapore, [9] noted two peaks between 40 to 49 years and 60 to 69 years, whereas Lavrnic et al., from former Yugoslavia, reported two peaks between 20 to 40 years and 70 to 80 years. [11] However, Mantegazza et al., [12] and Poulas et al., [6] reported a single peak in the females in the third decade and second and third decades respectively. In the studies from India, Saha et al., from Kolkata and we found a single peak of age at onset in females in the third decade. [13] In the male patients, Renato Mantegazza et al., from Italy reported a bimodal onset with the peaks in the third and sixth decade. [12] However, in several studies there is a single peak of age at onset in males. Poulas et al., [6] reported the peak in the sixth and seventh decade while Lavrnic et al., [11] reported in the sixth to eighth decade. In the present study we observed a single peak in the males in the sixth and seventh decade. In most studies [6],[13] including ours, the peak of onset has been earlier in the females as compared to males. The MGFA classification of the acquired group identifies subgroups of patients with myasthenia gravis who share distinct clinical features or severity of disease. [14] Ocular symptoms are frequent as the initial presentation. Mantegazza and Guidetti reported a frequency of 39.3% and 36.8% respectively. [12],[15] In our series 220 (26.31%) had ocular myasthenia. Respiratory distress can be a presenting feature of myasthenia gravis. In the series reported by Mantegazza 0.8% presented with respiratory symptoms. [12] There were 11(1.32%) patients in the present series who presented with respiratory muscle weakness requiring intubation. In patients undergoing thymectomy, nonthymomatous pathology is more common than thymoma. [16],[17],[18],[19] However, in several studies on thymic pathology in myasthenia from India, thymoma was found to be more common than thymic hyperplasia. [20],[21],[22] In the present study, the most common histopathology noted was thymoma. This is in all probability the consequence of selection bias as patients who underwent thymectomy had enlarged thymus on imaging or had more severe disease. Thymoma was more common in the males. Hyperplasia was more common in females. In many reported series thymomas are more frequent in the males. [17],[23] The present study has limitations as it is a hospital-based study. An epidemiological study would be useful to provide accurate answers to many questions raised such as male preponderance and to know if the prevalence in India is on the rise. Conclusion Myasthenia gravis in our study was more common in males. There was a single peak of age at onset in both males and females: in males in the sixth to seventh decade and in females in the third decade. AchR antibodies were positive in nearly 84% of the patients where it was tested. RNS was positive in 76% of the patients. The higher prevalence of thymomas in this series is in all probability due to selection bias as patients with thymic enlargement and more severe disease underwent thymectomy. Thymomas were more common in males and thymic hyperplasia in females.Acknowledgments We are grateful to Dr B K Goyal, Dean, Bombay Hospital Institute of Medical Sciences for allowing us to use the medical records. We are grateful to Dr Khushnuma Mansukhani and Dr Bhavna Doshi for doing the electrophysiological studies and late Professor John Newsom-Davis and Dr D Beeson for genetic studies. We thank Dr Nemish Shah and Dr Prakash Patil for doing the thymectomies.References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08087f3.jpg] [ni08087f1.jpg] [ni08087f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}