 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 56, No. 4, October-December, 2008, pp. 444-449 Original Article Cryptococcal meningitis in HIV infected: Experience from a North Indian tertiary center Susheel Kumar, Ajay Wanchu, Arunaloke Chakrabarti 1 , Aman Sharma, Pradeep Bambery, Surjit Singh Departments of Internal Medicine and 1 Microbiology, PGIMER, Chandigarh, India Correspondence Address: Dr. Ajay Wanchu, Department of Internal Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India. awanchu@yahoo.com Date of Acceptance: 26-Jun-2008
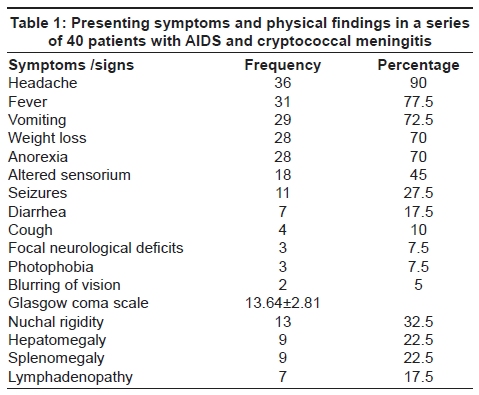
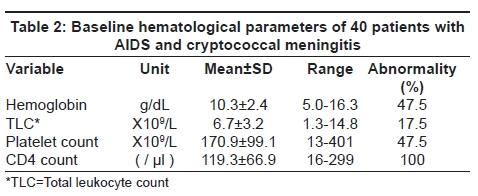
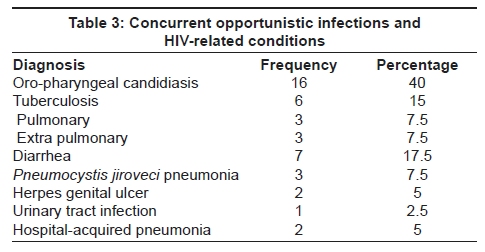
Code Number: ni08105 Abstract Background: Cryptococcal meningitis is a common opportunistic infection in Human Immunodeficiency Virus (HIV)-infected individuals. There is little information specifically addressing cryptococcal meningitis in HIV-infected patients from North India. Aims: To determine clinical presentation, hospital course, response to treatment, complications developed, in-hospital mortality, any recurrence of cryptococcal meningitis and reasons of recurrence during follow-up. Settings and Design: A retrospective observational study undertaken in a large tertiary care center. Materials and Methods: Patient's demographic data, presenting clinical symptomatology, physical findings, laboratory parameters, cerebrospinal fluid (CSF) examination findings, side-effects of treatment, development of any complications and hospital outcome were analyzed. During follow-up any recurrence of cryptococcal meningitis, possible reasons of recurrence, type of treatment received, complications developed and outcome was recorded as well. Results: Forty patients diagnosed to have cryptococcal meningitis were analyzed. Twenty-two (55%) patients had acute/ subacute presentation. Thirty-six (90%) patients presented with headache and 18 (45%) had altered sensorium. Twenty (50%) patients had no cells in the CSF. Hypoglycorrhchia was seen in 30 (75%) patients. Cryptococcal meningitis was the first acquired immune deficiency syndrome (AIDS)-defining illness in 30 (75%) patients. Thirty-five patients developed some adverse effects to amphotericin-B. Thirty-three patients improved with treatment while three patients died. Four patients had recurrence of cryptococcal meningitis within six months of first episode. Non-compliance of fluconazole therapy was the reason for recurrence in all of these patients. Conclusions: Cryptococcal meningitis is a common initial AIDS-defining illness. Acute and/or subacute presentation of cryptococcal meningitis is not uncommon in HIV-infected individuals. An early diagnosis of HIV infection might reduce the incidence of this infection.Keywords: Cryptococcal infection, HIV, immunocompromised, India, meningitis, outcome Introduction Human Immunodeficiency Virus (HIV) infection was first reported in India in the state of Tamil Nadu in 1986. [1] This infection has since spread to the entire country. According to official estimates in 2006, adult HIV prevalence was 0.36% and 2.5 million were infected with the virus. [2] The most common opportunistic infection in HIV patients in India is tuberculosis. [3],[4],[5],[6] Cryptococcal meningitis has been reported as the most common opportunistic infection of the central nervous system (CNS) of Indian patients with HIV infection. [3],[4],[5] Cryptococcal meningitis caused by environmental fungus Cryptococcus neoformans , is a common opportunistic infection in HIV-infected individuals, particularly in Southeast Asia, Southern and East Africa. [7] It usually infects HIV-infected patients with CD4 count < 100 cells/µl. These patients present with features of acute, subacute or chronic meningitis or meningoencephalitis. This infection is fatal without treatment. Therefore, rapid diagnosis and treatment is required to decrease fatality. Combination of amphotericin-B and flucytosine is the recommended initial treatment for the first two weeks. Fluconazole is started after two weeks of combination therapy. [7],[8],[9] Mortality from developed countries, secondary to HIV-associated cryptococcal meningitis is in the range of 10-30% while in developing countries the mortality rate is substantial, around 13-40% because of late presentation, limited access to antifungal therapy, and inability to adequately monitor intracranial pressure among many other reasons. [7] Since there is little information specifically addressing cryptococcal meningitis in HIV-infected patients from the Indian subcontinent, we carried out this analysis. Materials and Method This retrospective observational study was carried out at the Post Graduate Institute of Medical Education and Research (PGIMER) Chandigarh, a tertiary care referral hospital in Northern India. The catchment area of this hospital includes Chandigarh union territory and the adjacent states of Himachal Pradesh, Punjab, Haryana, Uttrakhand, Uttar Pradesh and Jammu-Kashmir. Patients presenting with cryptococcal meningitis between January 2005 and March 2008 were studied. Cryptococcal meningitis was defined as clinical features of meningitis/meningoencephalitis along with positive cerebrospinal fluid (CSF) cryptococcal antigen test or positive CSF India ink preparation or isolation of Cryptococcus neoformans in the CSF culture. Patients presenting with clinical features of meningitis/meningoencephalitis of less than four weeks duration were defined as having acute or subacute presentation. Patient's demographic data, risk factors for acquisition of HIV infection, prior acquired immune deficiency syndrome (AIDS) defining conditions, other concurrent infections, presenting clinical symptomatology, physical findings, laboratory parameters, CSF examination findings, side-effects of treatment, development of any complications and hospital outcome were analyzed. All patients received amphotericin-B (0.7 mg/kg/day) for two weeks. Flucytosine was not given as it was not available. Fluconazole (400 mg/day) was given for the next six weeks. Subsequently, secondary prophylaxis with fluconazole (200 mg/day) was continued till the CD4 count had increased to more than 200/mm 3 for ≥ six months. Follow-up data of these patients after discharge was recorded. During follow-up any recurrence of cryptococcal meningitis, possible reasons of recurrence, type of treatment received, complications developed and outcome was recorded as well. Various laboratory abnormalities were defined using cutoff values as follows: anemia - hemoglobin < 10 g/dL; leucopenia - TLC < 4 x 10 9 /L; thrombocytopenia - platelet count < 150 x 10 9 /L; hypoalbuminaemia - albumin < 3.5 g/dL; hyponatremia- plasma sodium< 135 mEq/l hypokalemia - plasma potassium < 3.5 mEq/L; hypomagnesaemia- plasma magnesium< 1.5 mg/dL; impaired renal function- blood urea nitrogen > 50 mg/dL and/or serum creatinine > 1.2 mg/dL ; elevated liver enzymes -> 2 times the upper limits of normal [aspartate aminotransferase (AST) -> 100 IU/L, alanine aminotransferase (ALT) -> 100 IU/L]. The following criteria were used to define common concomitant infections: Pulmonary tuberculosis (PTB): clinical features suggestive of TB with radiological features compatible with TB on chest radiograph or computed tomographic (CT) scan and/or demonstration of acid-fast bacilli (AFB) in sputum smears or growth of Mycobacterium tuberculosis in sputum culture. Disseminated tuberculosis (DTB): clinical features suggestive of TB with concurrent involvement of at least two non-contiguous organs, in the presence of bacteriological and/or histopathological evidence of TB and improvement with anti-tuberculosis therapy. Pneumocystis jiroveci pneumonia (PCP): bilateral, diffuse interstitial infiltrates on chest radiograph or high-resolution CT, with hypoxemia (PaO 2 < 12 kPa) and sputum smears/cultures negative for aerobic bacteria and AFB and/or demonstration of Pneumocystis jiroveci in induced sputum. Statistical analysis Statistical analysis was done using the statistical software 'SPSS version 13.0' (SPPS Corp, Chicago, IL, USA). Descriptive analysis consisted of mean with standard deviation and range for various parameters. Frequency of various clinical and laboratory findings and the frequencies of individual opportunistic infections are expressed as percentage. Results Forty patients diagnosed to have cryptococcal meningitis were analyzed. These included 35 males. Mean age of these patients was 40.0 ± 9.1 years. Most patients were in the age group of 25-49 years. Thirty-six (90%) patients presented with headache. Duration of headache ranged from two to 365 days. Fifteen patients had severe headache, while 12 patients had moderate and nine had mild severity of headache. Thirty-one (77.5%) patients had history of fever during presentation. Duration of fever ranged from one to 730 days. Twenty-two (55%) patients had acute/ subacute presentation of cryptococcal meningitis. Eighteen (45%) patients had altered sensorium. Duration of alteration of sensorium ranged from one to 15 days. Focal neurological deficit occurred in three patients. Eleven patients had history of seizures. All of them had generalized tonic-clonic seizures. Detailed clinical symptoms and signs of these patients during the time of presentation are shown in [Table 1]. Twenty-one (52.5%) patients were from the high risk groups including truck drivers and intravenous (IV) drug abuser. An identifiable risk factor for HIV infection was present in 21 (52.5%) patients. The commonest mode of transmission was multiple heterosexual unprotected sexual contacts, seen in 19 patients. One patient each had history of unsafe blood transfusion and intravenous drug abuse. Detailed baseline hematological parameters are shown in [Table 2]. CT scan head was done in all patients. Four patients had features to suggest communicating hydrocephalus, two patients had cerebral edema. One CT scan showed features of cerebral atrophy. Bilateral basal ganglia hypodensity, left basal ganglia hypodensity and ring-like enhancing lesion in left frontoparietal region was seen in one patient each. Twenty (50%) patients had no cells in CSF examination. Lymphocytic predominance was seen in 55% of the remaining 20 patients. The rest of the 45% patients had predominant polymorphonuclear response. Hypoglycorrhchia was seen in 30 (75%) patients. Eighteen patients had elevated CSF protein. India ink was positive in 34 patients. Cryptococcal antigen test in CSF was positive in all patients. Thirty-six (90%) patients had CSF culture positive for Cryptococcus neoformans . The CD4 cell count ranged from 16 to 299 cells/µl. Median CD4 cell count of the whole group was 109 cells/µl. Cryptococcal meningitis was the first AIDS-defining illness in 30 (75%) patients. Other infective conditions concurrently seen in 21 patients have been shown in detail in [Table 3]. Twelve patients had past history of infections which included TB in 10 patients, herpes zoster in two and cytomegalovirus (CMV) retinitis in one patient. Out of 17 patients receiving antiretroviral therapy (ART), 14 were receiving it at presentation. It was initiated within the last six months of index presentation in four of these patients. The remaining three were started on ART at the completion of two weeks of amphotericin-B. Six patients were receiving a combination of lamivudine, stavudine and nevirapine. Another six patients were receiving stavudine, lamivudine and efaviranz. Zidovudine, lamivudine and nevirapine combination was prescribed in three and two patients were receiving combination of zidovudine, lamivudine and efaviranz. Duration of ART in those patients already on treatment at the time of presentation ranged from 14 days to six years. All patients received conventional amphotericin-B (0.7 mg/kg/day) for initial two weeks and then were started on fluconazole (400 mg/day). Thirty-five patients developed some adverse effects to amphotericin-B. Commonest side-effect was hypokalemia seen in 29 patients. Acute febrile reaction occurred in 19 patients despite premedication with paracetamol and antihistaminics. Increase in urea and creatinine was seen in 11 patients. Hypomagnesaemia was seen in six patients, hyponatremia in five and anemia in four patients. Out of 40 patients, 33 patients improved with treatment while three patients died. Four patients left against medical advice and in all of these patients progressive deterioration in various clinical and biochemical parameters were seen during hospital stay. All three patients who died had objective evidence of raised intracranial tension. One of them also had altered sensorium at presentation. Four patients who left against medical advice had alteration of sensorium at presentation which continued to progress during hospital stay despite amphotericin- B therapy and other supportive measurements. Two of them had objective evidence of raised intracranial tension in the form of papilledema on fundus examination and diffuse cerebral edema on CT head and two of them also acquired hospital infection leading to progressive worsening of condition. Patients who improved received consolidation therapy with high-dose fluconazole (400 mg/day) for the next six weeks. Duration of follow-up in these patients ranged from 21 to 800 days. Mean duration of follow-up was 364.8 ± 234.1 days. Fifty per cent patients had a follow-up of more than one year duration. Mean number of visits per patients were 5.9 ± 4.2. All patients who were not receiving ART previously were started on ART four weeks after completion of two weeks amphotericin-B induction therapy. Four patients had recurrence of cryptococcal meningitis. All these patients had recurrence of cryptococcal meningitis within six months of the first episode. Non-compliance of fluconazole therapy was the reason for recurrence in all these patients. All except one patient responded to repeat therapy with amphotericin-B. Discussion Most of the patients were in the age group 25-49 years and males dominated the study group. This is in consonance with the technical report providing national level statistics published by National AIDS Control Organization (NACO) in the year 2006. [2] Triad of headache, fever and vomiting were predominant symptoms, similar to the earlier reports in the literature. [7],[8],[10],[11] Cryptococcal meningitis usually presents in the form of chronic meningitis. In this series more than half the patients had acute to subacute presentation. Our findings emphasize that even with acute presentation with features of meningitis in HIV-infected individuals, possibility of cryptococcal meningitis must always be considered and patients must be investigated accordingly. Alteration of sensorium was seen in 45% patients as compared with other studies showing this in 13-73% of patients. [10],[11],[12],[13],[14],[15],[16],[17],[18] Seizures have been reported in 9-35% of these patients. [10],[11],[18] In this study, 27.5% of patients had seizures. Focal neurological deficit was seen in a small number of patients, which is in consonance with other case series. [10],[11] Commonest associated infections were oral candidiasis and TB which are in consonance with two large studies on HIV-infected patients reported from the Indian subcontinent. [3],[4] In a significant percentage of patients in this case series, cryptococcal meningitis was the initial AIDS-defining illness which is comparable to that seen in South African and Zambian studies. [11],[17],[19],[20] An identifiable risk factor for HIV infection was seen in half of study group. Heterosexual mode was the commonest mode of transmission of HIV infection. The possible reasons for not revealing the source of infection or high-risk behavior could be prevailing social values which forbid any sexual relationship other than heterosexual mode, not wanting to disclose his/her personal information etc. Due to the immunocompromised status, CSF has high load of cryptococcal organisms and less of inflammatory response leading to lower white cell counts in HIV-infected patients. [10],[11],[13],[14] Thus, India ink is positive in 70-90% of AIDS patients and in only 50% of non-AIDS patients. [7],[8] In our patients, 50% (20) patients had no white blood cell in CSF and 85% (35) patients had India ink test positive. Hypoglycorrhchia was seen in 75% of patients. Detection of cryptococcal capsular polysaccharide antigen is an important test in diagnosing this infection. Various studies have shown overall sensitivities and specificities of this test in the range of 93-100% and 93-98% respectively. False positive results of this test are approximately 0-0.4%. [7],[8] All our patients had positive cryptococcal antigen test done in CSF. The CD4+ T cell count is the best indicator of the immediate state of immunologic competence and also the strongest predictor of HIV-related complications in these patients. Cryptococcal infection was the major opportunistic infection and a major cause of death in HIV-infected patients with CD4 cell count < 100 cells/µl in the pre-highly active antiretroviral therapy era. [8] In one study the average CD4 lymphocyte count in patients with AIDS and cryptococcosis was 73 cells/µl. [21] Median CD4 cell count in this case series was 109 cells/µl. The immune reconstitution inflammatory syndrome (IRIS) is a spectrum of clinical signs and symptoms resulting from the restored ability to mount an inflammatory response associated with immune recovery. The incidence of IRIS was 10-32% in various studies on HIV patients being initiated on ART. [22],[23],[24] Clinical events occurring before the first six months of ART therapy often represent IRIS related to preexisting conditions. In this series, out of 14 patients receiving ART at presentation, four patients receiving ART for six months or less presented with features of cryptococcal meningitis possibly indicating IRIS. Median CD4 cell count of these patients was considerably lower (79 cells/µl) as compared to the whole group (109 cells/µl). The remaining 10 patients were receiving ART for more than six months. The development of a new or recurrent World Health Organization (WHO) Stage 3 or 4 condition after the first six months of ART is considered functional evidence of HIV disease progression. This finding of the present study has important implications and these patients developing opportunistic infection after six months of ART should be the focus of investigations to exactly pinpoint cause of treatment failure, which because of the retrospective nature of this study was not feasible. Untreated cryptococcal meningitis is uniformly fatal. A large randomized controlled trial undertaken by Mycoses Study Group established the combination of amphotericin-B deoxycholate (0.7 mg/kg/day) and flucytosine (100 mg/kg/day) as a standard of care for the treatment of cryptococcal meningitis in AIDS patients. [25] The findings of this study were further substantiated by another study. [26] In this case series, due to unavailability of flucytosine, amphotericin-B (0.7 mg/kg/day) was used alone. In a substantial proportion of patients (87.5%), some adverse effects due to amphotericin- B were noted. These side-effects were managed with premedication, adequate hydration and electrolyte replenishment and were easily treated. None of them was life-threatening. All the patients in this study group ultimately received complete therapy with amphotericin-B. In-hospital mortality in this case series was 7.5%. Out of the patients followed up, one patient died during the initial 10 weeks of follow-up. There was no recurrence of cryptococcal meningitis after six months of follow-up. The National Institute of Allergy and Infectious Diseases Mycoses study group and AIDS clinical trials group showed 5.5% mortality at the end of two weeks and 9.4% mortality at the end of 10 weeks with combination therapy of amphotericin-B and flucytosine. [25] In another study, mortality was 14% at two weeks and 22% at 10 weeks. [26] One study from Thailand showed 16% mortality at two weeks and 24% mortality at four weeks in patients who received high-dose amphotericin-B only for two weeks followed by oral azole therapy. [27] From South African countries, in most of the studies only fluconazole had been used as monotherapy for cryptococcal meningitis and mortality in these studies is disappointingly high. [11],[17] The poor prognostic factors are depressed level of consciousness, signs of raised intracranial pressure, depressed CSF cell counts and glucose levels and CSF cryptococcal antigen titer > 1024. [28] The most important of all the poor prognostic factors is the CSF opening pressure with values ≥ 250 mm H 2 O. [29] Our observations reemphasize the prognostic importance of alteration of sensorium and raised intracranial tension in these patients as the majority of patients having poor outcome had these poor prognostic factors. In conclusion, this study demonstrates acute and/or subacute presentation of cryptococcal meningitis in more than half of HIV-infected individuals. In 75% of patients cryptococcal meningitis was the initial AIDS-defining illness. Four patients receiving ART for six months or less presented with features of cryptococcal meningitis possibly indicating IRIS. Ten patients receiving ART for more than six months had developed cryptococcal meningitis indicating failure of current ART regime. CSF examination besides showing poor inflammatory response had hypoglycorrhchia in 75% of patients possibly indicating higher organism load. High-dose 'amphotericin-B Only' induction therapy followed by fluconazole consolidation therapy yielded acceptable results. High-dose amphotericin-B resulted in reversible side-effects in a substantial proportion of patients and in none of them these were life-threatening. Alteration of sensorium and raised intracranial tension are poor prognostic factors in these patients. Recurrence of cryptococcal meningitis was seen in the initial six months of follow-up and noncompliance of medication was the reason for recurrence in all of these patients. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08105t2.jpg] [ni08105t1.jpg] [ni08105t3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}