 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 56, No. 4, October-December, 2008, pp. 463-470 Original Article Dysphagia in acute stroke: Correlation with stroke subtype, vascular territory and in-hospital respiratory morbidity and mortality Uma Sundar, Vimal Pahuja, Nishant Dwivedi, Murar E. Yeolekar Department of Medicine, Neurology Sub-Divison, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, India Correspondence Address: Dr. Uma Sundar, House No-58, Bharat Tirth Co-operative Housing Society, Sion Trombay Road, Chembur, Mumbai - 400 071, India. umasundar2@rediffmail.com Date of Acceptance: 18-Apr-2008
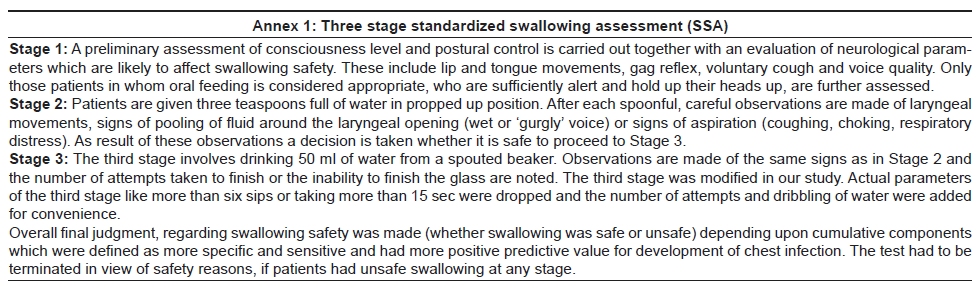
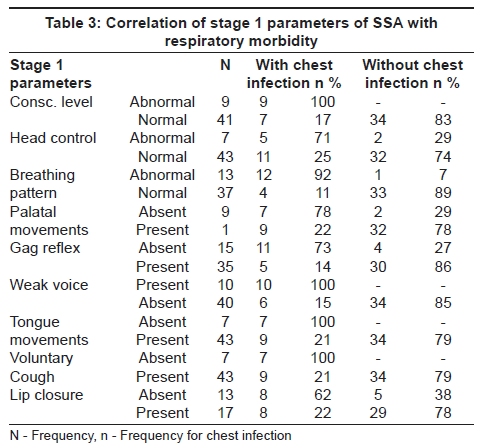
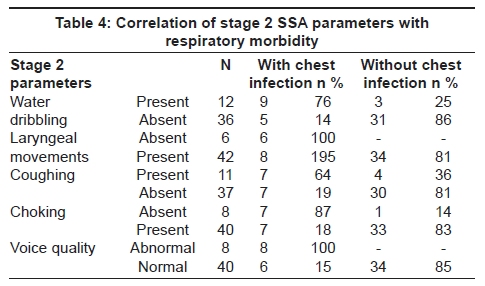
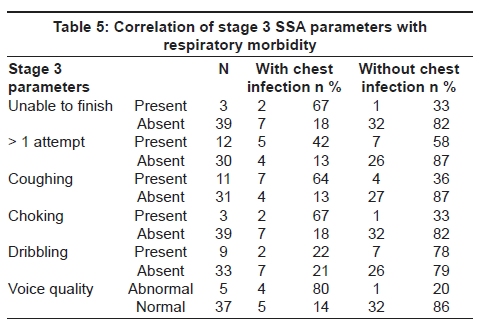
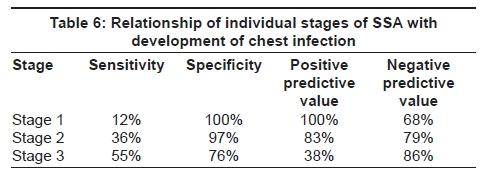
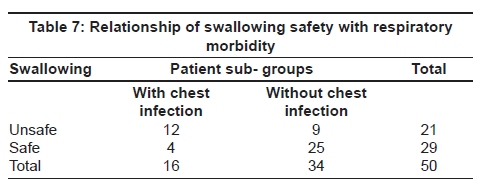
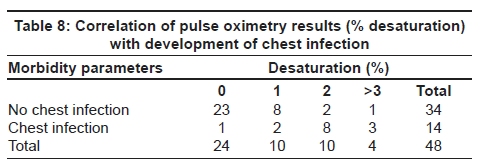
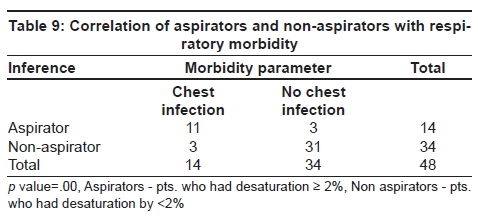
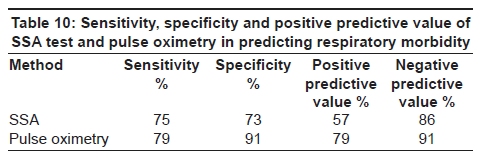
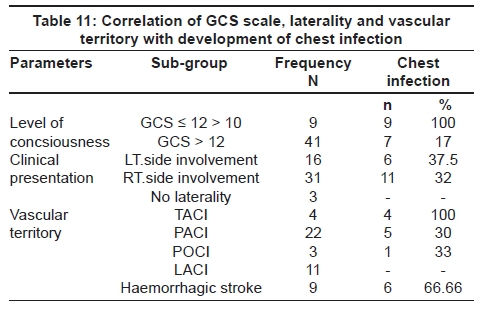
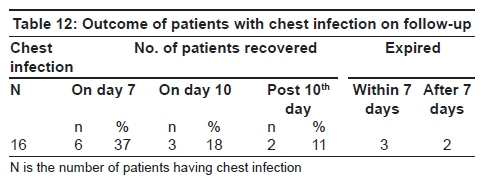
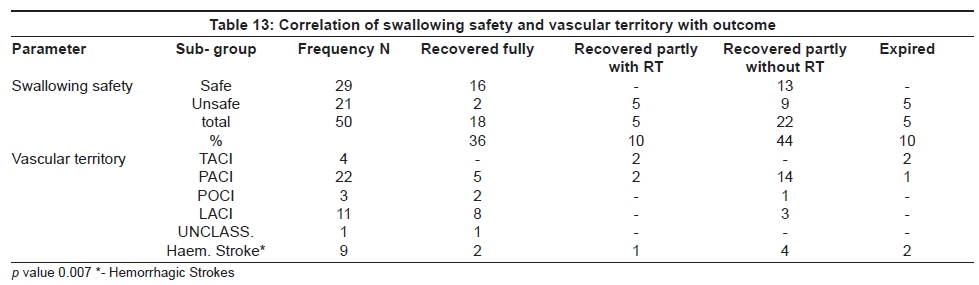
Code Number: ni08108 Abstract Aims: The study aimed at correlation of post-stroke dysphagia with area and volume of infarct/ bleed, and with subsequent in-hospital respiratory morbidity and mortality. Materials and Methods: 50 patients of acute stroke were serially recruited. Standard Staff swallowing assessment was performed within 24 hours of admission along with pulse oximetry. Ischemic strokes were classified as per OCPS registry. In-hospital respiratory morbidity and mortality, mode of nutrition and disability status at discharge were noted. Results: 21/50 (42%) patients had post-stroke dysphagia during their hospital course. Among infarcts, Total Anterior Circulation Infarcts (TACI) had 100% incidence of dysphagia, followed by Partial Anterior Circulation Infarcts (PACI-36%), Posterior Circulation infarcts (POCI-33%), and Lacunar infarcts (LACI-18%). 67% of hemorrhages had post-stroke dysphagia. Staff swallowing assessment had a sensitivity and specificity of 75% and 73% respy., for predicting respiratory morbidity. The corresponding figures for Pulse oximetry were 79% and 91%.Keywords: Dysphagia, stroke, respiratory morbidity. Introduction Swallowing dysfunction complicates acute strokes in 25-32% cases [1] and directly affects patients' prognosis and recovery. [2],[3],[4] Dysphagia was earlier hypothesized to result only with bi- cortical involvement or brainstem affection. [5],[6],[7],[8] However, it is now proven that unilateral hemisphere affection can also cause dysphagia. [9],[10],[11],[12],[13],[14] Dysphagia complicates the course of acute strokes through its potential of development of chest infection, nutritional problems and dehydration. [15],[16] Patients with dysphagia are more likely to require care in rehabilitation centers. [17] Dysphagia is also an independent predictor of respiratory morbidity and mortality in acute stroke. [18],[19] In this prospective study, the aim was to correlate the presence of dysphagia following stroke with the vascular territory involved along with volume of infarct/hemorrhage. The aim was also to determine morbidity and mortality in patients having dysphagia following stroke and to determine the predictive value of individual parameters in the Standardized Swallowing Assessment [20] {SSA} (Annex - 1), (a bedside test used for assessing dysphagia) for prediction of chest infection. We also aimed to determine the value of dysphagia for predicting respiratory morbidity and subsequent mortality in acute stroke. Materials and Methods The study was carried out in a tertiary care teaching hospital. Fifty patients, admitted within 48 h of acute stroke were serially recruited. Patients with glasgow coma score (GCS) less than 10, poor postural control (thus unable to sit up for SSA) and patients presenting after 48 h of onset were not included. Standard clinical neurological examination and imaging were performed and patients were classified according to Oxfordshire Community Stroke Project (OCSP) clinical classification in the case of infarcts. [21] The SSA was carried out in all patients within 24 h of admission. Pulse oximetry (MICROMON 7142L) (Annex - 2) was performed simultaneously with Stage 2 and 3 of SSA. Patients with desaturation ≥ 2% from baseline were judged as aspirators. Results of pulse oximetry were double-blinded. All patients were monitored daily for development of chest infection. The parameters checked were tachypnoea (RR>22/min), tachycardia, fever, inspiratory crackles/bronchial breathing, antibiotic use, X-ray evidence and hypoxia on ABG. Presences of three or more findings were taken as indicators of chest infection. [17] The mode of nutrition during hospital stay and discharge (Intravenous, Ryle's tube (IV, RT) oral) was noted. The final outcome was studied in terms of recovery from chest infection and dysphagia and neurological recovery. Patients with residual neurological deficit and dysphagia at discharge were labeled as having partial recovery with nasogastric tube dependence. Those with only neurological deficit and no dysphagia at discharge were labeled as having partial recovery. Statistical analysis The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of each SSA parameter for predicting respiratory morbidity was assessed with 2x2 tables. The sensitivity and specificity of SSA in its entirety and pulse oximetry for assessing dysphagia was calculated as per standard formulae. The Pearson's and Chi-Square test were utilized for correlating unsafe swallowing with respiratory morbidity as well as final outcome of patients. Results Forty-one of 50 patients had infarcts, the majority among them (44%) being Partial Anterior Circulation Infarcts (PACI) as per the OCSP classification. Twenty-two per cent had Lacunar Infarcts(LACI), 8% Total Anterior Circulation Infarcts (TACI) and 6% Posterior Circulation Infarction (POCI). Of the nine hemorrhagic strokes seven were subcortical. All nine patients with GCS < 12 had unsafe swallowing. Only 12 of 41 patients with GCS > 12(29%), had swallowing difficulty ( p < 0.05). Non-dominant hemispherical affection was seen in 16 (32%) patients and 10 (62%) of them developed dysphagia. [Table - 1] correlates vascular territory with swallowing safety. All patients with TACI had dysphagia; 36% of PACI, 18% of LACI and one patient in the POCI group had dysphagia. One patient who could not be classified in any subgroup, remained free of dysphagia. In [Table - 2] swallowing safety in cortical and subcortical infarcts was analyzed. Of 11 patients with cortical infarcts seven had unsafe swallowing, four of these seven having dominant lobe infarction. Of the four cortical infarcts with safe swallowing, two had affection of the dominant lobe. Sixty per cent of patients with non-dominant hemisphere and 66% of dominant hemisphere involvement, developed dysphagia; 63% of all cortical infarcts developed dysphagia. In contrast only 21% (six out of 29) of patients with subcortical infarcts developed dysphagia. The profile of unsafe swallowing in subcortical infarcts was as follows: 2/9 basal ganglia infarcts, 1/4 thalamic, 1/9 internal capsule infarcts and 2/3 brainstem infarcts had dysphagia. Four patients (corona radiata, centrum semiovale) had safe swallowing. The volume for hemorrhagic stroke (seven subcortical, one cortical, one quadrigeminal cistern) was correlated with dysphagia. Six of seven subcortical bleed patients had dysphagia with hemorrhage volume ranging from 3.3 to 8.4 cc. The single cortical bleed (volume 32.4 cc) had dysphagia. [Table - 3] shows that in Stage 1, the consciousness level (GCS < 12), abnormal breathing pattern, weak voice, absent/decreased tongue movements and poor voluntary cough had 100% positive predictive value for predicting chest infection. Impaired gag reflex had sensitivity of 69% and specificity of 88% and low positive predictive value of 73% but good negative predictive value of 86%. Impaired lip closure had sensitivity and specificity of 50% and 85% respectively, for predicting chest infection. [Table - 4] reveals that in Stage 2, impaired laryngeal movements and poor voice quality had sensitivity of 64% and 57% respectively and 100% specificity and positive predictive value for predicting chest infection. Water dribbling during swallowing had good negative predictive value (86%). 'Poor coughing' had good specificity of 88%, low positive predictive value (64%) but good negative predictive value (81%) for development of chest infection. [Table - 5] shows that in Stage 3, inability to finish 50 ml of aliquots, 'poor voice quality' and 'choking on fluids' had higher specificity of 97% and good negative predictive value of 82% with positive predictive value of 67%. Cough in Stage 3 had almost similar sensitivity and specificity as in Stage 2 (29% and 79%) with poor positive predictive value of 22%, but had good negative predictive value (87%) in determining the risk of development of chest infection. [Table - 6] shows that the positive predictive value of Stage 1 for chest infection is high. In Stage 2 specificity was 97% but positive predictive value dropped to 83%. Stage 3 has highest negative predictive value but low sensitivity and specificity (55% and 76%) to predict chest infection. [Table - 7] shows correlation of swallowing safety with development of chest infection. In all, 16 patients developed chest infection. Twelve of these belonged to the unsafe swallowing group (21). In the safe swallowing group, four out of 29 developed chest infection. This difference was significant by applying Chi-square test. The overall rate of infection in a group of patients who had swallowing abnormalities was 57%. [Table - 8] reveals that out of 24 patients who had no desaturation, only one developed chest infection. Two out of 10 patients with 1% desaturation had chest infection. Ten patients had desaturation by 2%, out of which eight showed signs of chest infection. Three out of four patients who had> 3% desaturation, developed chest infection. [Table - 9] shows that chest infection with desaturation of ≥ 2% was seen in 11 out of 14 patients (78.5%). Three aspirators (who had desaturation ≥ 2% on pulse oximetry) did not develop any chest infection. Aspiration and desaturation by ≥ 2% was found to be significant in the development of chest infection by applying Chi-square test. The SSA test, devised as a bedside tool to predict chest infection, was sensitive enough to predict development of chest infection (75%) and had good specificity (73%) with positive predictive value of 57%. Pulse oximetry which is also a bedside tool has sensitivity of 79% and a high specificity of 91% with positive predictive value of 79% and negative predictive value of 91% [Table - 10]. [Table - 11] shows that level of consciousness predicted the incidence of chest infection in 100% patients. Patients who had left-sided involvement had 37.5% chances of development of chest infection whereas patients with right-sided involvement had 32% chances of development of chest infection. Patients without any lateralizing signs did not develop chest infection. All the patients with TACI developed chest infection, whereas none of the patients in the LACI group had signs of chest infection. In the hemorrhage group, six out of nine patients (66.66%) had respiratory morbidity; 5 out of these 6 patients had subcortical bleeds and one had cortical bleed. [Table - 12] reveals the analysis of patients suffering from chest infection. It was evident that all developed chest infection within three days of hospital stay. Out of these, six (37%) patients recovered at one week. Three patients expired within seven days, seven patients went on to have infection for more than seven days out of which two expired. Three patients (18%) recovered on the 10th day and two patients continued to remain morbid because of chest infection. One out of these two recovered on the 14th day. [Table - 13] shows that correlating swallowing safety with outcome revealed that five out of 21 patients (24%) in the unsafe swallowing group had residual dysphagia. Five (24%) patients in the unsafe swallowing group expired. There were nine patients who recovered from dysphagia during the hospital stay and two had full recovery in this group. The patients in the safe swallowing group (n=29) did not show any mortality during their course; 16 of them recovered fully and 13 patients recovered with partial neurological deficit. Results of correlation of vascular territory with outcome show that all patients in the TACI group had poor outcome (two patients had residual dysphagia with RT feeding at discharge and two expired). Fourteen out of 22 patients (63.6%) in the PACI group recovered partially neurologically and had no dysphagia, while two patients had dependency at discharge. Five out of 22 patients in the PACI group recovered fully. Recovery was good in the LACI group with 8 out of 11 patients recovering completely. In patients who had posterior circulation involvement (n=3), two patients had good recovery. One recovered without any dysphagia but had neurological deficit. These results were significant i.e. unsafe swallowing influences the outcome of patients with stroke. The nutritional support of the patients in the 'unsafe group' (21), included IV fluids in 19 patients and RT feeding in seven patients. None among the safe group had RT feeding. The 'unsafe swallowing' group required admission for a mean of 10.8 days and 'safe group' for 6.5 days. Discussion Dysphagia following acute stroke is a common and serious problem. Contrary to earlier belief that brainstem and bicortical involvement only can lead to dysphagia it is being increasingly recognized now that unilateral hemispherical affection can cause dysphagia. [5],[6],[7],[8],[19] Byrun and Gathier [13] discussed reports of lower precentral gyrus and posterior part of the inferior frontal gyri that caused a cortical form of pseudobulbar palsy with dysphagia, "the operculum syndrome". Of all stroke patients with dysphagia, 37-54% aspirate, 38% develop chest infections and 3.8% die of pneumonia following stroke. [22],[23],[24] Dysphagia being an independent marker of post-stroke morbidity and mortality, [17],[19] it is important to identify swallowing dysfunction in stroke early. Although video fluoroscopy is the gold standard for swallowing assessment, [25] the SSA has been proven to be easier to administer, comparably effective with less risk to patients and with higher negative predictive value as compared to video fluoroscopy. [26] In this study of 50 patients, 21 were detected to have dysphagia on SSA. Level of consciousness was significantly related to dysphagia. Nine out of 21 'dysphagic patients' had GCS < 12. Of these nine patients, two were eliminated in Stage 1 SSA and six in Stage 2. Consciousness has a major impact on the integrity of the swallowing mechanism. The initial stages of swallowing are controlled by voluntary mechanism governed by facial, tongue and pharyngeal movements which are bound to be affected by altered sensorium. The later stages which are largely involuntary are controlled by subcortical mechanisms which may be affected by basal ganglia, thalamic, large hemispherical or bihemispherical lesions. [27] In this study all patients with GCS< 12 and 29% of alert patients (GCS>12) had swallowing problem. In a study by Ellul et al ., [20] in post-stroke patients, 70% patients with 'drowsy with arousable state' developed dysphagia, whereas only 29% of alert patients were similarly affected. Similar results were also noted by Barer et al . [14] In this study 62% of non-dominant hemispherical lobe developed dysphagia . However, the impact of dominant lobe affection on dysphagia cannot be commented upon, as the majority of patients had subcortical strokes (29/41). Barer DH [14] has shown the presence of post-stroke dysphagia in 32% of patients with dominant hemispherical lobe involvement versus 27% patients with non-dominant hemisphere involvement. It appears that unilateral affection of either lobe, dominant or non-dominant can result in dysphagia, contrary to the earlier belief that only bihemispherical lesions where supratentorial structures are concerned, could lead to dysphagia. [19],[27] TACI had 100% propensity to develop dysphagia [Table - 1], possibly related to large area of hemispherical infarction. Lacunar strokes showed the lowest incidence of swallowing dysfunction, probably correlating with small infarct volume and better collateral circulation through circle of Willis. The findings are comparable with the Ellul et al . study, [20] and it can be inferred that patients with TACI are at greatest risk of developing dysphagia. On analysis of subcortical infarcts with dysphagia [Table - 2], brainstem strokes had the highest incidence. This is due to lower motor involvement of bulbar swallowing mechanisms and possibility of reticular system involvement. In studies by Horner et al . [28] and De Pippo et al ., [29] 65% and 66% of brainstem strokes respectively developed dysphagia. To judge the swallowing safety at individual stages of SSA it is essential to identify those parameters which are sensitive, specific and good predictors of chest infection to substantiate our judgment of safe/unsafe swallowing at each stage. In Stage 1 consciousness level, abnormal breathing pattern, weak voice, decreased tongue movements and poor cough were very specific parameters to indicate the development of chest infection and thereby unsafe swallowing. However, each of these parameters has significantly lower sensitivity, if considered individually. In Stage 2, poor laryngeal movements and voice were highly specific and predictive of chest infection, whereas 'lack of choking and water dribbling' had high negative predictive value for chest infection. In Stage 3, voice quality remains the parameter with fair negative and positive predictive value (PPV), both 80%. Coughing, choking and 'inability to finish the glass' had better negative predictive value {NPV} (80%). In assessing patients from Stage 1 to Stage 3 it is evident that the earliest stage had highest PPV and specificity but low sensitivity to predict chest infection. Therefore patients judged to have 'unsafe swallowing' at SSA 1 had 100% chance of developing chest infection, but 'safe swallowing' at SSA 1 did not rule out risk of respiratory morbidity as NPV was 68%. Stage 2 specificity and PPV were lower (97% and 83%) as compared to Stage 1, however NPV was 79%. Stage 2 assessment of patients was better in predicting that a normal parameter would lead to normal respiratory function. Stage 3 had higher NPV (86%) substantiating this finding. The early stages evaluate more obvious and gross abnormalities, as compared to the later stage, where more subtle and discrete dysfunction is assessed. Hence "failing the earlier stage would have high PPV for predicting respiratory morbidity". Even at the end of Stage 3, 4/29 patients who were judged to be safe developed respiratory morbidity. These were possibly 'silent aspirators'. Pulse oximetry was performed on all except two patients, who were eliminated in SSA 1, GCS being less than 12. Aspirators were found to be at a significantly higher risk of development of chest infection. Pulse oximetry desaturation while swallowing, was a good predictor of subsequent respiratory morbidity in this study with specificity of 91%. These findings were comparable with studies by Zaidi et al . [30] and Collins et al ., [31] who also confirmed oxygen desaturation on swallowing as a marker of aspiration in acute stroke. On attempting to correlate pulse oximetry desaturation with failure of SSA, the following was noted: in Stage 2, all SSA failed patients had desaturation ≥2%. Of those six patients eliminated at this stage, all desaturated by ≥2% and five developed chest infection. Nine out of 42 patients who were carried forward at Stage 2, developed chest infection eventually and only 2/9 (22.22%) patients had desaturation by ≥2% at this stage. In Stage 3, 5/13 patients judged to be having unsafe swallowing, developed chest infection. All five patients desaturated by ≥2%; 4/25 patients judged to be having safe swallowing developed chest infection out of which one patient desaturated by ≥2%. Thus, 22.22% of the patients who developed chest infection despite clearing SSA 2 and 25% of patients who developed chest infection despite clearing SSA 3, were in reality identified as 'silent aspirators' on pulse oximetry over and above the SSA. As expected, level of consciousness correlated directly with respiratory morbidity, all patients with GCS 10-12, developing chest infection. This, evidently, was 'through unsafe swallowing' as all these patients had been demonstrated to have dysphagia. The laterality of neurological deficit did not appear to influence the respiratory morbidity. As expected all TACI patients had respiratory morbidity, again correlating with all of them having unsafe swallowing. The figures for chest infection in PACI, POCI and LACI were comparable to figures for dysphagia in these groups. Analyzing the outcome of patients with chest infection, mortality was seen both during the early and interim period and was closely related to unsafe swallowing and low GCS. Correlation of vascular territory and final outcome clearly indicates that patients with TACI were more morbid, dysphagia being persistent during discharge and recovery being incomplete. The TACI group also had 50% mortality. Patients of lacunar stroke had the best results for complete recovery. These findings are comparable to the Ellul et al ., [20] study showing 49% mortality and 45% dependency in TACI patients and 4% mortality and 30% dependency in the LACI group. Thus TACI infarcts appear to have the worst outcome with respect to both mortality and dependency at discharge, as compared to other groups, most likely because of the extent and volume of hemispherical involvement. [Table - 13] shows that of 29 patients who had safe swallowing, none expired and none had dependency at discharge, whereas 50% patients of the 'unsafe swallowing' group either expired or were dependent on discharge. Thus, a significant correlation between unsafe swallowing and morbidity, mortality and dependency at discharge could be concluded. Conclusions Dysphagia is a common and serious problem in stroke patients and affected 21 out of 50 recruited patients in this study. Hemorrhages (67%) and cortical infarcts(68%) had higher propensity to develop dysphagia, with TACI having 100% incidence of developing swallowing dysfunction in the infarct subgroup, followed by PACI (36%) and POCI (33%), with the LACI (18%) group being the least affected. In the subcortical stroke group six out of 29 patients (21%) had swallowing problems. The SSA, employed as a bedside tool for detecting dysphagia revealed that in Stage 1 level of consciousness, weak voice, voluntary cough and absent tongue movements had 100% PPV for prediction of chest infection. In Stage 2 absent laryngeal movements and abnormal 'voice quality' had 100% PPV for predicting chest infection. In Stage 3 abnormal 'voice quality'(86%), coughing and unable to finish the glass (87% each) in one attempt had good negative predictive values. Overall, SSA as a screening method, had sensitivity of 75% and specificity of 73% to pick up chest infection. Pulse oximetry showed sensitivity of 79% and specificity of 91% to predict chest infection. SSA failure and desaturation ≥ 2% on pulse oximetry, correlated significantly with respiratory morbidity, subsequent mortality and 'dependency status' at discharge. The presence of TACI infarcts correlated significantly with subsequent respiratory morbidity and mortality. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08108a1.jpg] [ni08108t10.jpg] [ni08108t9.jpg] [ni08108t6.jpg] [ni08108t2.jpg] [ni08108t12.jpg] [ni08108a2.jpg] [ni08108t8.jpg] [ni08108t1.jpg] [ni08108t11.jpg] [ni08108t5.jpg] [ni08108t13.jpg] [ni08108t3.jpg] [ni08108f1.jpg] [ni08108t4.jpg] [ni08108t7.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}