 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 56, No. 4, October-December, 2008, pp. 477-479 Case Report Congenital irreducible atlantoaxial dislocation associated with cervical intramedullary astrocytoma causing progressive spastic quadriparesis Anooj Chatley, Awadesh K. Jaiswal, Manoj Jain1 , Sanjay Behari Departments of Neurosurgery and 1 Pathology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India Correspondence Address: Dr. Sanjay Behari Department of Neurosurgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India. sbehari@sgpgi.ac.in Date of Acceptance: 09-May-2008
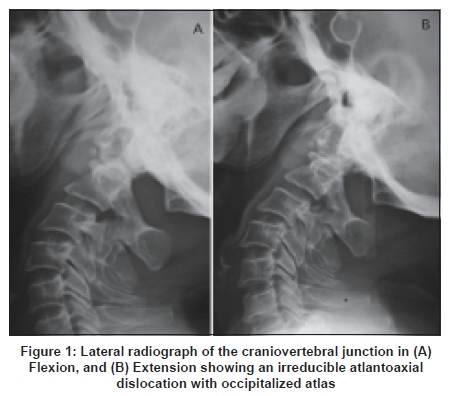
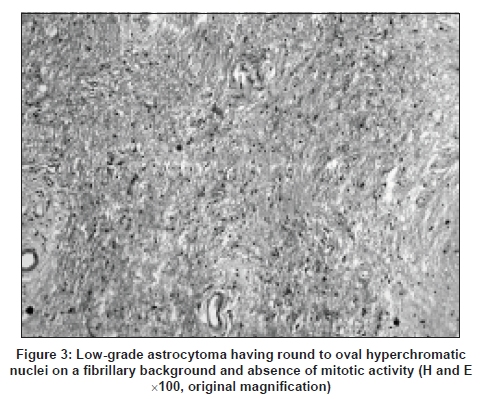
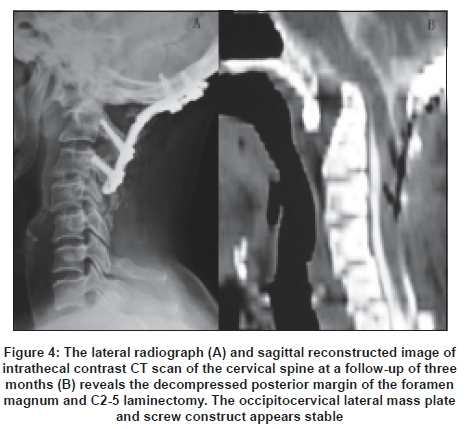
Code Number: ni08111 Abstract Simultaneous presence of congenital irreducible atlantoaxial dislocation (AAD) and cervical intramedullary astrocytoma has not been previously described and may cause disabling myelopathy. This 55-year-old lady presented with suboccipital pain, spastic quadriparesis, Lhermitte's phenomenon and sphincteric disturbances. Lateral radiographs and magnetic resonance imaging showed irreducible AAD, occipitalized atlas, C2-3 fusion, and,an intramedullary tumor from C2-5 level iso-to-hypointense, non-enhancing, except in a small segment in the dorsal C2 level. A suboccipital craniectomy with C2-5 laminectomy revealed a greyish-white tenacious tumor. The tumor was decompressed using a C2-5 midline myelotomy and duroplasty. An occipitocervical lateral mass fixation was performed. Histopathology revealed a low-grade astrocytoma. At three-month follow-up, her spasticity had decreased and quadriparesis and sphincteric disturbances were persisting. Postoperative lateral radiographs and intrathecal contrast CT scan showed a stable occipitocervical construct. Thus, the suboccipital craniectomy and laminectomy with midline myelotomy and duroplasty facilitated space for progressively expanding intramedullary astrocytoma with irreducible AAD; the lateral mass fixation provided stability at the craniovertebral junction.Keywords: Atlantoaxial dislocation, intramedullary tumor, spinal cord astrocytoma. Introduction We report a rare case having congenital irreducible atlantoaxial dislocation (AAD), occipitalized atlas and C2-3 fusion associated with a cervical intramedullary low-grade astrocytoma leading to progressive spastic quadriparesis with sphincteric dysfunction. The radiological features and surgical strategies for simultaneously dealing with the two entities are described. Case Report A 55-year-old lady presented with suboccipital pain, progressive spastic quadriparesis and Lhermitte's phenomenon with hesitancy and precipitancy of micturition for one year. On examination, she had wasting of left forearm flexor, thenar and hypothenar muscles, spastic quadriparesis Grade IV and absence of left triceps and supinator jerks with hyperreflexia of all other deep tendon jerks. Her plain lateral radiographs of the craniovertebral junction (CVJ) in flexion and extension [Figure - 1A] and [Figure - 1B] and T1-weighted magnetic resonance (MR) image revealed an AAD with occipitalized atlas, C2-3 fusion, asymmetrical occipito-C1-C2 lateral joints with a C2 to C5 level iso- to mildly hypointense tumor [Figure - 2A]. On T2-weighted images, foramen magnum narrowing was associated with T2 intramedullary signal changes at C1-2 level. The cord was expanded by a dorsal, hyperintense lesion that extended from the mid C2 vertebral body level to C5-6 disc level [Figure - 2B] with a small area of contrast enhancement at C2 level [Figure - 2C]. The MR intensity pattern suggested a C2-C5 spinal cord astrocytoma. At surgery, in prone position, a suboccipital craniectomy and a C2-5 laminectomy were performed. The expanded spinal cord had a grayish, tenacious avascular appearance. After C2-5 midline myelotomy, tumor decompression was done using ultrasonic suction aspirator. A duraplasty was performed using a fascia lata graft. Then, bilateral occipito-cervical Vertex plates and screws (Meditronics) contoured to the occipitocervical curvature with onlay bone grafts were fixed under fluoroscopic guidance to the occiput and C1-2 lateral masses. The patient was kept on overnight elective ventilation. The histopathology revealed a low-grade astrocytoma having round to oval hyperchromatic nuclei on a fibrillary background and absence of mitotic activity [Figure - 3]. At follow-up after three months, her spasticity had decreased, her quadriparesis and left upper limb wasting and sphincteric disturbances were persisting. Her postoperative lateral radiograph of the cervical spine [Figure - 4A] and sagittal reconstructed images of intrathecal contrast computed tomographic scan [Figure - 4B] revealed the decompressed posterior margin of the foramen magnum and C2-5 laminectomy with a stable occipitocervical construct. Discussion Pathogenesis and radiological features The congenital irreducible AAD in our patient was associated with other occipital and upper cervical sclerotomal defects like assimilated atlas, C2-3 fusion and asymmetrical occipitocervical facet joints. [1],[2] The recurrent flexion-extension of the neck causing tenting of the upper cervical cord against the posteriorly directed odontoid; the assimilated and stenosed atlantal canal diameter leading to foramen magnum compromise; and, the diffusely infiltrating low-grade astrocytoma expanding the cord from the C2-C5 level were all responsible for the progressive myelopathy that our patient developed. [1],[2],[3],[4] An intramedullary ependymal cyst at the C2-3 level with associated irreducible AAD causing spastic quadriparesis has been previously reported. The cyst was well-circumscribed with characteristic cerebrospinal fluid (CSF) density and non-enhancement on contrast. [5] Goel et al ., have reported a "waist-like" syringomyelia (with CSF-like intensity) in three infants having mobile and congenital AAD. They cautioned that in atleast two of these cases, the syringomyelia was earlier diagnosed to be an intramedullary tumor. [6] The syrinx was present in the center of the cord with well-defined margins, mainly at the C1-2 level; and, at the site of maximum bony compression showing the "waist". [6] In our patient, however, the C2-5 astrocytoma was below the level of the coexisting AAD. It was nearly isointense to the cord on T1-weighted images, more dorsally placed, and without a clear demarcation from the normal cord. The T2-weighted image showed its infiltrative nature; and, at the upper end of the lesion, there was a characteristic contrast enhancement. The diffusion weighted images showed a hyperintense signal indicating a solid tumor rather than a syrinx. The small nodular enhancement seen in our patient may also be seen in patients harboring spinal cord hemangioblastomas or granulomas. [3],[4] In the latter cases, cord expands both below and/or above the lesion; and, the intensity of the cord at the level of the widened segments does not differ from that of the normal cord. In our patient, however, the T2-weighted images showed the focal cord expansion to be distinct from the normal cord. In the present study, majority of the intramedullary astrocytoma was non-enhancing. Similar non-enhancing astrocytomas have been reported in approximately 9% of patients with long-segment spinal cord tumors. [7],[8] The small enhancing portion in the cord has as differential diagnosis an inflammatory lesion, multiple sclerosis or acute disseminated encephalomyelitis. [8] Surgical considerations Irreducible AAD is addressed by transoral decompression [2],[9],[10] and posterior stabilization, usually under the same anesthesia. [9],[10] In our patient, however, only posterior decompression of the foramen magnum and assimilated atlas along with C2-5 laminectomy were performed. The intact subarachnoid space anterior to the cord at the C1-2 level despite the T2 cord intensity changes indicated that dynamic neck movements rather than canal compromise was responsible for myelopathy. Thus, occipitocervical stabilization obviated the possibility of further cord trauma by the posteriorly directed odontoid during flexion and extension movements at the neck. The C1-2 lateral mass provided adequate ground for purchase of screws in the presence of suboccipital craniectomy and C2-5 laminectomy. [1] The "two-stage" strategy for radical resection of intramedullary tumors was utilized for addressing the intramedullary tumor. [4] According to this, in the first stage, the midline myelotomy provides the cavity for the poorly-defined tumor to occupy. The tumor filling the myelotomy site may subsequently be safely excised without causing significant postoperative deficits. Thus, tumor decompression was done using suction aspirator but no attempt was made to radically extirpate the tumor considering its strategic location, infiltrative nature and lack of a well-defined plane of cleavage. A duroplasty ensured further space for the cord to expand. This surgical strategy has resulted in a temporary alleviation of progression of myelopathy. Radiotherapy has been deferred due to the low proliferative potential of the lesion. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08111f4.jpg] [ni08111f2.jpg] [ni08111f3.jpg] [ni08111f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}