 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 56, No. 4, October-December, 2008, pp. 493-494 Letter To Editor Cytomegalovirus polyradiculopathy: A rare neurological manifestation of acquired immunodeficiency syndrome Anant Mohan, Duncan Smith-Rohrberg1 , M. Sethu, S. K. Sharma Department of Medicine, All India Institute of Medical Sciences, New Delhi-110 029, India, Correspondence Address: Department of Medicine, All India Institute of Medical Sciences, New Delhi-110 029, Inida surensk@gmail.com Date of Acceptance: 09-May-2008
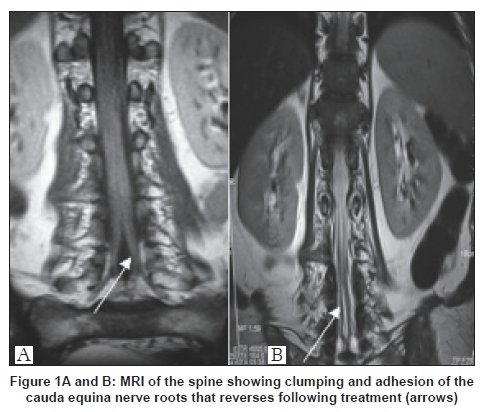
Code Number: ni08122 Sir, Polyradiculopathy is a rare but potentially devastating syndrome more common in Acquired Immunodeficiency Syndrome (AIDS). Although cytomegalovirus (CMV) is most commonly implicated, the differential diagnosis includes tuberculosis, syphilis, and lymphoma. We admitted a 36-year-old army truck driver from Haryana, India, HIV-positive since May 2004, with ascending, asymmetric flaccid paraplegia, lower extremity paraesthesia, and bladder and bowel retention since three months. His CD4 count was 4 cells/µl. He received intravenous (IV) immunoglobulin, oral Gancyclovir and highly active anti-retroviral therapy (HAART) comprising Zidovudine, Lamivudine, and Nevirapine, without improvement. On examination, all muscles of the lower extremity were hypotonic, wasted, with 0/5 strength, and absent deep tendon reflexes. Bulbocavernous and anal reflexes were absent. Light and deep touch sensations, nociception, proprioception, and vibration sense was all diminished bilaterally extending superiorly to approximately the L1 dermatome. Cerebrospinal fluid (CSF) showed 40 polymorphonuclear leukocytes per µl, 336 mg/dL protein, 90 mg/dL glucose (CSF: serum 62%), and negative on gram, India ink, and acid-fast bacilli staining. Suspecting polyradiculopathy due to cytomegalovirus or tuberculosis (TB), both intravenous Gancyclovir and anti-tuberculosis treatment (ATT) were initiated along with HAART. Magnetic resonance imaging (MRI) of the spinal cord showed confluent arachnoiditis of the cauda equine [Figure 1A]. CSF was sterile and CSF polymerase chain reaction (PCR) for mycobacterium and CMV were negative. Anti-CMV IgG was strongly positive in serum; blood testing for anti-CMV IgM, anti-HSV IgG/IgM, VDRL for syphilis, anti-toxoplasma IgG/IgM, HBsAg, and anti-HCV were all negative; CSF for anti-CMV IgM/IgG, anti-HSV IgG/IgM, VDRL, and PCR for TB and CMV were negative. The patient gradually improved, and a repeat MRI after one month showed marked improvement in the confluent nerve roots [Figure 1B]. At three months follow-up, the patient was taken off Gancyclovir, and had recovered> 50% of motor, sensory, and bladder and bowel function. He became ambulatory and tendon reflexes normalized. The final clinical impression was that of AIDS-related CMV polyradiculopathy that failed to respond to oral Gancyclovir but responded well to IV Gancyclovir and HAART. Polyradiculopathy in AIDS is a rare but devastating syndrome. This report, to the best of our knowledge, is the first such report from the Indian subcontinent. The differential diagnosis includes CMV, [1],[2] tuberculosis, Varicella zoster virus, Ebstein Barr virus, Herpes simplex virus, syphilis, and lymphoma. CMV causes a subacute, progressive, asymmetric ascending paraplegia with urinary retention and sacral dysesthesias. Initial CSF examination in CMV may reveal the "classic" pattern of polymorphonuclear pleocytosis, elevated protein, and decreased glucose in only 50%. Nucleic acid amplification techniques are often rapid, sensitive, and specific, though expensive. In our case PCR for CMV was negative in CSF; although this test generally has sensitivity greater than 80%, [3] prior treatment decrease yield. Detection of CMV antigens (pp65) in CSF has a sensitivity of 91% and specificity approaching 100%. [4] Histopathological examination of the cauda equina roots shows polymorphonuclear or mononuclear inflammation with CMV inclusions in Schwann cells and endothelial cells. Treatment is usually empirical with IV Gancyclovir. Foscarnet may be used in rare cases of Gancyclovir-resistance. [5] Response to therapy may be assessed by a repeat lumbar puncture after two weeks. Prolonged IV initiation therapy with subsequent oral maintenance may be required. Finally, even if a viral etiology is highly likely, the clinician may choose to initiate ATT, especially in India. All together, three classes of etiological agents may be targeted in the HIV-positive subacute progressive polyradiculopathy patient: HIV, tuberculosis, and the herpesviridae family. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08122f1.jpg] |
| |||||||||

{kind=link}